| |
April
2015
- Volume 9, Issue 2
Training community based nurses in impoverished areas of developing
countries: A practical solution to a rapidly emerging global
shortage of health workers force

|
 ( (
|
Manzoor
Butt
Correspondence:
Dr
Manzoor Ahmed Butt
Rawalpindi,
Pakistan
Email: drmanzoor@ymail.com
|
|
|
Background
The developing countries of the world face a chronic
shortage of medical doctors, nurses and skilled health
care workers. This is truer about women's health care
workers because many women do not prefer to be examined
and managed by male health workers due to their religious,
social and cultural reasons. Health workers are the
heart and soul of health systems. A new progress report
[1] estimates a global shortage of 7.2 million health
workers, with 83 countries facing a health worker crisis.
The relative shortages of doctors, nurses and midwives
are still most acute in sub? Saharan Africa. This is
currently one of the major obstacles to achieving the
MDGs [2] and other international health goals including
universal health coverage. The following graph depicts
fertility and mortality in various regions of the world
[3]. If we intend to change the dire situation in Sub-Saharan
Africa, South Asia, Middle East & North Africa,
and elsewhere, we have to enroll and train existing
and new Nurses and other health care workers for primary
and secondary health care.
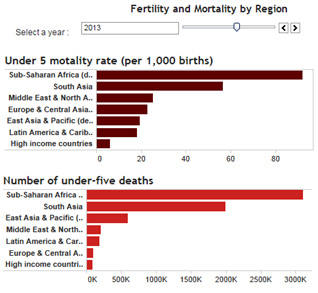
Source: [3]
Pakistan has an organized infrastructure for delivering
health care even in small villages but there is an extreme
lack of nurses and health care workers. There is one
doctor, one nurse and one bed for 1400, 3261 and 1531
people respectively. 76% deliveries occur at home [4].
The main part of budget allocated for health goes to
teaching institutions and major hospitals of federal
and provincial capitals; very little is left for towns
and small villages.
Like many developing countries, ours is a male dominant
society where only very few females enjoy full rights
and have access to opportunities
of even very basic human needs. This is even more true
in the health sector, where unfortunately there is a
great lack of female doctors and nurses combined with
a large number of female 'quacks' in the country. The
female doctors are neither easily available nor easily
affordable and women do not prefer to be examined by
male doctors. There are a lot of government hospitals
which provide free or low fee treatment to women but
those are not preferred because of: [6]
- The casual and offhand behaviour
of doctors
- More than one male doctor examining the patient at
one time
- The fear of crowds of medical students present at
time of examination
- The fear that doctor may misuse this opportunity for
some evil deed
Formal and qualified nurses are not willing to work
in small cities, towns and villages.
They prefer government hospitals of federal and provincial
capitals. This is justified if they work in a proper
manner on merit on rotational basis but this seldom
happens. They use all means to stay in these hospitals
until someone more resourceful replaces them.
|
Introduction
This article describes the importance of training locally
existing non formal nurses / health care workers in developing
countries with Pakistan as an example. If we have to overcome
the shortage of nurses / health care workers, we have to include
those who are already in field. It would be easier to educate
and train them as compared to only including new ones. The
author has used his own example to indicate and prove that
it is possible to include non formal nurses and train them
towards formal training course.
Present situation in Pakistan
To understand the exact situation in Pakistan, we have to
concentrate on basic health statics. The following figures
are taken from Global Health Observatory [5]
Click here for
Figure 2: Basic statistics
Click here for Figure
3: Utilisation of health services
Click here for
Figure
4: Millenium development Goals
The access of people to medical facilities
varies greatly from very privileged to absolutely devoid.
Both the government and private health services are available
to people. Our upper and middle classes have full access to
government as well as private health facilities. The real
problem is with the masses and the people who live below the
poverty line.
What does the term nurse mean in Pakistan
The following categories are usually included under this term;
1) Classified Nurse: The female must have passed high
school examination in science to get admission into this course.
She takes a four years course in Nursing during which she
has to reside in hospital. Due to proper education and training,
they work ethically and are aware of importance of working
in own limits.
2) Lady Health Visitor (LHV): The female must have
passed high school examination in science to get admission
into this course. She takes a short course of about two years
and she is basically trained in women's health and midwifery.
3) Lady Health Worker (LHW): This type was produced
by government to induce health education and create awareness
about women's health. They are usually only middle pass and
a local resident.
4) Locally Trained Nurses: This is the most available
variety. Some of them are high school graduates but most of
them are usually middle passed or less. They are neither adequately
educated nor properly trained.
5) Midwives or Traditional Birth Attendants (TBA):
In Pakistan, TBAs are usually uneducated and non-trained.
81% of deliveries are conducted by them.
6) Community based Midwives : They are enrolled and
trained by UNICEF through its partner institutions. They are
hope for future.
The health care delivery system and
needs of the population are changing rapidly
A major part of our budget goes to defense needs. Despite
all efforts for reduction of poverty, more and more people
are going below the poverty line. Our population is growing
rapidly. There is a rapidly increasing burden on the government
funded health care system. There would be an increasing need
of health care workers, especially the nurses. We have to
shift more care from hospital to primary care; most important
in this context is Health Education, Mother and Child Health,
Family Planning and Contraception, Immunization, Infection
control and other disease control.
The total population of Pakistan (in thousands) was 141,256.2
in the year 2000. It would be 181,384.7 in the year 2010 and
227,781.1 in the year 2020. Total Numbers of people (from
age group 0 to 60+ years) requiring daily care was 8,292.1(in
thousands) in the year 2000. It is expected to be 10,908.2(in
thousands) in 2010 and 14,254.5 (in thousands) in year 2020.
This means the total Numbers of people (from age group 0 to
60+ years) requiring daily care would increase by 32% in the
year 2010 and 72% in the year 2020 as compared to year 2000
[7]
The role of nurses in the delivery of primary
care
The community based nurses and health workers play the largest
part in the delivery of primary care. They are the first contact
of people who not only seek their help for primary care but
also in acute emergencies and accidents.
The emerging challenges to nurses
There is an urgent need to train and organize the nurses and
health Workers.They have to play a vital role in the delivery
of primary care in coming years because of tendency of people
to avoid hospitals. Non formal nurses / health workers lack
adequate knowledge and skills especially regarding antenatal
care and safe childbirth. They have to address their shortcomings
by adopting professional development strategies and CME. The
practical way is to induce these trainings at jobs.
What is the solution
The author describes his efforts and strategy to address the
problem of shortage of skilled nurses and health care workers
in his community in this section. He devised and launched
a program for organization and training of local nurses and
health Workers in antenatal care in his community-----Shamsabad,
Rawalpindi.
Object of the program
1- To evolve a platform for training of existing and new nurses
/ health workers on CME pattern.
2- To create and maintain a "Data Base" of existing
and new nurses / health workers so that all recent knowledge
and skills could be conveyed to them.
3- To evolve an easy to understand manual in local language
for education and training of existing and new health workers
4- To help the nurses / health workers to evolve their own
organizations that could strive for them in accordance with
the following guideline principals of WHO ;
i) Cater for their education& training
ii) Provide support and protection to them
iii) Enhance their effectiveness
iv) Tackle imbalances and inequalities
Who would benefit by this program
Our doors are open for all existing and new nurses / health
workers. We are specially focusing
on locally available nurses initially but we will help all
regardless of their age, gender, race, religion, creed and
method of treatment. All health concerns like doctors, nurses,
midwives, TBAs, Hakims, Homeopaths, laboratory technicians,
dental technicians, and community health workers are welcome.
The strategy for
Training
Step 1: Identification and registration of existing
and new nurses / health workers for training
Step 2: Determination of Extent of training
Step 3: To impart training
Step -4: To evaluate the candidates after completion
of training
The syllabus and extent of training
There are three levels of education and training (Primary,
secondary and tertiary) depending upon the extent of curriculum.
In author's opinion, every care provider must have very clear
understanding and skills of Monitoring of Vital Signs {Pulse,
BP, Temperature and Respiratory rate}, weight recording, Cardio-Pulmonary
Resuscitation, Sterilization and Asepsis.
Main syllabus
Nutrition, Anemia, Brief Anatomy (maternal & foetal),
Brief Basic knowledge about breast examination, Brief Basic
knowledge about Menstrual cycle , Family planning (both regular
& Emergency), Gynaecological examinations, Antenatal Care,
Rhesus incompatibility, Pre-Eclampsia, Eclampsia, CPR, Foetal
growth & well being, Vaginal bleeding during pregnancy
(Ectopic pregnancy, Miscarriage & abortion, Antepartum
Hemorrhage, Post Partum Hemorrhage, Placenta Praevia, accidental
Haemorrhage, Hydatidiform mole), Twin pregnancy, Labour (normal
& abnormal), Various methods of delivery (Normal delivery,
mal-positions, hygiene, avoiding trauma, analgesia, and danger
signs and how to manage hemorrhage), Postnatal care of mother
(Normal and danger signs such as endometritis, bleeding, Eclampsia),
Puerperium, Brief knowledge of D&C, E&C, Resuscitation
of newborn, Immediate Post-natal care of the child, breast
feeding, vaccination,. Etc
The extent of training
i) Primary Level of Training: This is mean for community
health workers. It would be in form of short and basic courses.
Incentives for learners: No big incentives are required; just
certificates of appreciations would be sufficient.
ii) Secondary Level of training: This is meant for
those who intend to adopt it as profession. Incentives for
learners: Certain incentives like certificates plus some financial
support in form of scholarship are necessary.
iii) Tertiary level of training: This is full and advanced
training to evolve life saving nurses. Incentives for learners:
Definite incentives like certificates, financial support during
learning plus employment opportunity are essential.
Conclusion
35.9% of the population lived in urban areas in 2010. 46.6%
or 29.9 million of the urban population live in slums.[8]
More people are shifting from rural to urban areas. The government
health care system is unable to cater for needs of all, especially
for those in rural and sub urban areas. There is shortage
of nurses that cannot be overcome by enrolling and training
new nurses. In author's opinion, the practical approach to
overcome the shortage of nurses in impoverished areas of developing
countries is to include already existing non formal nurses
in the community. They should be organized and trained through
CME approach and accommodated in health care delivery system
at community level. The author has success in addressing women
health problems at his community level through locally trained
nurses. [9] He also imported same training to community resource
persons (CRPs) from remote villages of the northern areas
( Chitral) of Pakistan. The results are more promising in
the remote areas than in main cities due to more need in those
areas. It is also very useful to use more pictographs than
text. Non formal nurses / health workers lack education, using
simple local language and descriptive images are the vital
part of training.
References
1) A Universal Truth: No Health Without a Workforce, Third
Global Forum on Human Resources for Health Report by Global
Health Workforce Alliance and World Health Organization, available
at: http://www.who.int/workforcealliance/knowledge/resources/hrhreport2013/en/
2) Millennium Development Goals, http://www.un.org/millenniumgoals/
3) Population estimates and projects, fertility and mortality,
region wise, World bank, available at: http://datatopics.worldbank.org/hnp/popestimates#
4) Position in 2004, Page-32, Population Growth & its
Implications-July 2004 by National Institute of Population
studies, Islamabad.
5) WHO Statical Profile, Pakistan; available at : http://www.who.int/gho/countries/pak.pdf?ua=1
6) Skilled Health Workers - A Solution to Primary Health Problems
in Pakistan, by Dr Manzoor Butt, available at: http://www.mejfm.com/journal/july2006/Skilled%20Health%20Workers%20-%20A%20Solution%20to%20Primary%20Health%20Problems%20in%20Pakistan.htm
7) Pakistan, Appendix 3: Sensitivity analysis. Numbers of
people requiring daily care, total population, proportion
of total population requiring care, and dependency ratio by
region, country and year, based on three severest Global Burden
of Disease study disability categories (levels 5, 6, 7). Source:
www.who.int/docstore/ncd/long_term_care/emro/pak.htm
8) Urban health profile, Pakistan, available at: http://www.who.int/kobe_centre/measuring/urbanheart/pakistan.pdf?ua=1&ua=1
9) Women's Health Problems in Pakistan, Dr Manzoor Butt. Available
at: http://www.mejfm.com/Newarchives2013/Women.pdf
|
 |

