| |
January
2015
- Volume 9, Issue 1
Breast
Cancer, Breast Self-Examination Knowledge among Female High
School Students in Riyadh City

|
 ( (
|
Kholoud M. Al-Haji (1)
Salma A.Moawed (2)
(1) Demonstrator, Department of Maternal & Child
Health Nursing,
College of Nursing , King Saud University, Riyadh,
Kingdom of Saudi Arabia
(2) Professor, Doctor, Department of Maternal &
Child Health Nursing,
College of Nursing , King Saud University, Riyadh,
Kingdom of Saudi Arabia .
Correspondence:
Kholoud M.Al-Haji , Department
of Maternal & Child Health Nursing,
College of Nursing , King Saud University, PO Box 1155149,
Riyadh 11758,
Kingdom of Saudi Arabia
Email: Kalhaji@ksu.edu.sa
|
|
|
Abstract
Breast cancer (BC) is the most prevalent form of cancer
in the Kingdom of Saudi
Arabia, accounting for 11% of all female cancers. It
is considered to be a progressive disease with a poor
prognosis if detected late. The low level of knowledge
and practice of breast self-examination is an important
method of prevention. The study was aimed at assessing
the knowledge of breast cancer and practice of Breast
Self-Examination (BSE) among female secondary school
students in Riyadh city.
Material & Methods : A cross-sectional descriptive
correlation design was used in this study. A representative
probability sample was recruited (Sample Size = 917
Students). A self-administered questionnaire was prepared
by the researcher. It consists of four parts. Data was
analyzed using the SPSS software package (version 16)
for data entry and analysis.
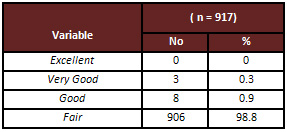
Results: The results of the study indicated that
none of the secondary school students had an excellent
knowledge regarding breast cancer; 98.8% of the participants
had a fair level of knowledge about breast cancer. The
mass media was the most common source of information
about breast cancer. The majority of participants did
not perform breast self-examination 80.8%; only 3.4%
perform (BSE) on monthly basis . There was a statistically
significant relation between level of breast cancer
knowledge and secondary school type, nationality, family
history of breast cancer and secondary school levels
but there was no significant relation between knowledge
of breast cancer and age groups, marital status and
family income level. Logistic regression analysis revealed
that a negative family history of breast cancer was
a significant predictor for lower scores on the level
of knowledge of breast cancer. However, age group, family
history of breast cancer were significant predictors
of performance of breast self-examination.
Conclusions : This study revealed that most of
the female secondary school students in Riyadh, Saudi
Arabia had very low knowledge about breast cancer. We
recommended developing a health educational program
about breast cancer for students, teachers and the community,
to raise awareness.
Key words : Breast cancer, Knowledge & Practice,
Secondary school.
|
Introduction
Breast cancer is the most common cancer among Arab women.
Breast cancer incidence rates in Arab women have increased
during the last 24 years, and women are now being diagnosed
with breast cancer at more advanced stages of the disease(1).
In 2008, the Saudi Ministry of Health reported that BC among
females constituted the highest percentage of cancers, 26.9%
of total number of malignant tumors in Riyadh and 31.9% in
Jeddah (2).
Young breast cancer patients have a lower rate of survival
than older breast cancer patients due to being diagnosed at
an advanced stage, but if discovered early breast cancer can
usually be cured, however, early detection through screening
is the only way to reduce mortality (3). The women who are
in the process of transitioning from adolescence to adulthood
offer a unique, critical window of opportunity for change
in (or impact on) health behavior.
Students in secondary schools, mainly teenagers, are considered
a vulnerable group passing through a critical period of physiological
and mental development that requires special health care.
The adolescent period is a time of rapid change that provides
teaching opportunities for shaping health behaviors into adulthood.
Teaching breast self-care may encourage positive behaviors
such as performing breast self-examination and seeking regular
professional breast examinations (5,6,7). Health behaviors
such as BSE can help empower women to take some control and
responsibility over their health promotion (4). For younger
women, BSE education and adherence to clinical breast examination
and mammography screening later in life provides for early
detection.
Educating young women about early diagnostic methods of breast
cancer is critically important to increase their breast cancer
awareness. Acquiring the behavior and practice of BSE at an
early age will also increase the probability of continuing
it later (8,9).
Regular performance of BSE does not mean that breast cancer
is necessarily self-detected. BSE increases body awareness,
so that there is heightened awareness of changes that may
be detected during BSE or at some other time. Although the
American Cancer Society, 2007 recommended that women beginning
in their 20s should be told about the benefits and limitations
of BSE, this procedure is not considered the best method for
early detection but the best option for interval screening
among women of all ages(8,10). The poor knowledge and wrong
beliefs about breast cancer prevention among teenagers are
responsible for a negative perception of the curability of
a cancer detected early and of the efficacy of the screening
tests.
Many studies have shown that nurses have positive influence
on women's breast cancer knowledge and BSE practice (11).
Women who were advised about BSE by health care providers
demonstrated greater knowledge, and confidence and were likely
to practice it routinely . Although there were a lot of studies
about knowledge of breast cancer and practice of BSE in female
university students (3,14,15 ), there were few studies about
the knowledge of breast cancer and practice of BSE in the
age group of 15-20 years (5,12). The role of the nurse ,therefore,
is to empower women by providing information, advice and support.
Breast cancer awareness includes knowledge of breast cancer
risk factors, signs, symptoms, and screening methods(12,13).
The objective of this study was to assess the knowledge of
breast cancer and Practice of Breast Self-Examination (BSE)
among female high school students in Riyadh city.
Material &
Methods
Study design: Cross-sectional descriptive correlation
design was used in this study.
Settings : The study was conducted at secondary girls'
schools, both governmental
and private in Riyadh city.
Study subjects : A representative probability sample
of secondary school girls, both Governmental and private in
Riyadh city was recruited for conducting this study. The total
number of the study subjects was 917 female students.
Sample criteria :
1- Inclusion criteria : Female secondary school students
in Riyadh city.
2- Exclusion criteria: Those who were absent or couldn't
complete the questionnaire for any reason.
Tools for data collection :
A self-administered questionnaire prepared by the researcher
after the review of literature was used. It consists of four
parts as following;
Part I :
1- Socio-demographic characteristics such as age, secondary
school type, marital status ….etc.
2- Personal and family history for breast cancer: It
is composed of 4 questions; the answers are ?Yes, No, or I
don't know.
Part II:
Knowledge of students about breast cancer composed of 5 questions
:
1- General knowledge about breast cancer: It is composed
of 4 questions; the answers are ?Yes, No, or I don't know.
2- Knowledge about the risk factors of breast cancer
was assessed by 11 questions, the answers were ?Yes, No, or
I don't know?. This part assesses the presence of breast cancer
risk factors with reference to guidelines of the American
Cancer Society (2008)(40).
3- Knowledge about the signs &symptoms of breast
cancer, it consists of 7 questions, the answers are ?Yes,
No, or I don't know..
4- Knowledge about the methods of early detection of
breast cancer, it consists of 5 questions, the answers are
?Yes, No, or I don't know.
5- Knowledge about the methods of breast cancer treatment,
it consists of 5 questions, the answers are ?Yes, No, or I
don't know.
Part III:
Knowledge about breast self-examination practice, it is composed
of 4 questions; the students were asked whether they performed
breast self-examination and if they answered ?yes, they were
asked some skills performed during their examination.
Part IV :
About source of information about breast cancer.
Ethical Consideration :
Permission was obtained from the Director of School Education
affiliating with the Ministry of Education after asking for
permission to carry out this study in 12 schools throughout
the academic year (2013/2014). The students who were given
information about the study and who accepted to participate
in the study were included. They were informed about the aim
and potential benefits of the study and their consent was
taken and their confidentiality was ensured.
Statistical analysis :
Data was analyzed using the SPSS software package (version
16) for data entry and analysis. Descriptive statistics with
cross -tabulations were performed. The Chi-squared test, was
used to examine the association between variables. Linear
regression models were used to assess the relation between
the demographic variables and level of knowledge.
Scores on knowledge level were predicted from the following
variables (7 predictors): school type (coded 1 = private,
2 = governmental), age groups (coded 1 = 15-16 yrs., 2 = 17-18
yrs., 3 = 19-20 yrs., 4 = more than 20 yrs.), nationality
(coded 1 = Saudi, 2 = non-Saudi), marital status (coded 1
= single, 2= married), secondary level (coded 1 = first, 2
= second, 3 = third), family income (coded 1 = good, 2 = medium,
3 = poor), family history (coded 1 = yes, 2 = No). The total
N was 917. The significance level used was being with p<
0.05.
For the total knowledge of breast cancer, the total score
was 38. A score of 0- 25 was considered a fair level of knowledge;
26-29 was considered a good level of knowledge, 30-33 was
considered a very good level of knowledge, while 34-38 was
considered an excellent level of knowledge. A score of 1 was
assigned to each correct answer while zero was assigned to
incorrect answer.
Results
Out of the 1000 questionnaires administered to the respondents,
917 were fully completed giving a response rate of (91.7%).
Table 1 shows the sociodemographic characteristics of the
participants. Most participants, 491 (53.5%), were aged between
17 and 18 years old. A majority of female secondary school
participants were from governmental secondary schools, (67.1%).
A greater percentage of secondary school participants were
Saudi citizens, (81.7%), while (18.3%) were non-Saudi participants.
A majority of female secondary school participants were single,
(98%). Little more than one half of the participants,(58.9%)
considered their financial status as medium between (5000-8000
SR).
Table 1: Distribution of the female students according
to their Socio-demographic Characteristics
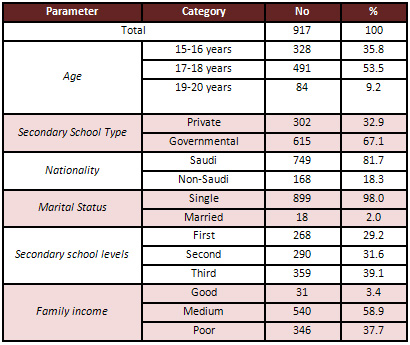
Table 2: Distribution of the female students according to
their total degree of Knowledge about Breast Cancer
The personal and family history related to breast cancer was
summarized in four questions. The first question was about
any previous problems in the breast; the majority of participants
did not complain of any breast problems. Only (8%) participants
complained of a breast problem. The second question was about
the history of breast surgery; the majority of the participants,
had no breast surgery. The third question was about family
history of breast cancer; the majority of participants have
a negative family history of breast cancer and only (6%) participants
had a positive family history of breast cancer. The fourth
question was about having a family history of other kinds
of cancers; (79%) had negative family history of other types
of cancers. while (12%) had positive family history of other
types of cancers.
Regarding general knowledge about breast cancer nearly half
of the samples (53.3%) answered not all breast tumors are
cancer while more than half of samples they did not know of
Metastasis (57%) and the causes of breast cancer(52.2%), and
if it can be prevented completely(43.3%).
Regarding the risk factors of breast cancer, the most widely
known risk factors for breast cancer was exposure to radiation
(41.9%), smoking (49.4%), but most of them didn't know the
association between breast cancer and late menopause (70.9%),
late age at first pregnancy (more than 30 years )(69.7%) early
menarche (less than 12 years.) (51%) , use of OCP (58.5%)
woman who do not breast feed 48.6% and eating fatty food 48.4%,
increasing age (47.5%) , obesity (44.3%).
Regarding knowledge about the signs and symptoms of breast
cancer, when they were asked about the symptoms the samples
answered correctly, the presence of a mass in the breast (66.6%),
sense of mass under the armpit (48.4%), pain in the breast
area (64%) are the warning signs of breast cancer, while more
than half of the sample did not know the warning signs of
breast cancer such as bloody discharge(50%), wrinkling in
the skin of the breast(57%) and inverted nipples (71.4%).
Concerning the screening methods for detection of breast cancer,
more than two thirds of the sample mentioned that blood test
(64%), breast exam by the doctor (78.3%), and breast self-examination
(70.4%) are the methods used for early detection of breast
cancer, while one third of the participants have information
about mammography (38.5%) and magnetic resonance imaging of
the breast (38.3%).
Regarding the line of treatment of breast cancer, more than
half of the samples (52.1%) mentioned that surgical treatment
is only the method of treatment and less than half of sample
(48.4%) mentioned chemotherapy is the treatment while more
than two -thirds did not know that radiotherapy (64.3%) hormonal
therapy(67.3%), and immunotherapy(67.4%) are methods of treatment
of breast cancer.
Regarding the knowledge of breast self-examination practice,
Table 3, the majority of samples (86%) don't know how to do
BSE . Only (2.3%) participants were doing breast self-examination
on a regular basis and (16.9%) performing it on a non-regular
basis, while (80.8%) did not perform breast self-examination.
(3.4%) participants were doing breast self-examination once
per month. A small percentage of the students had knowledge
about appropriate time for BSE (5.1%).
Table 3: Distribution of the female students according
to their Knowledge about Breast Self-Examination Practice
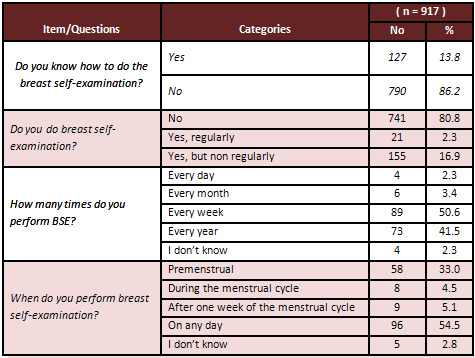
Table 4: Results of Chi-square test significance for variables
with degree of knowledge with breast cancer
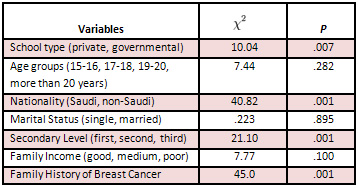
The association between demographic variables and degree
of knowledge of breast cancer for female students
A chi-square test was used to test the
association of breast cancer knowledge level with secondary
school type, age group, nationality, marital status, secondary
school levels, and family income Table 4. The variable of
secondary school type (private school) (x2=10.04,
P=.007) was significantly associated with level of knowledge
of breast cancer. The variable of nationality (Saudi) (x2=40.82,
P=.001) was significantly associated with level of knowledge
of breast cancer. The variable of secondary school level (first)
(x2=21.10, P=.001) was significantly
associated with level of knowledge of breast cancer. The variable
of family history of breast cancer (x2=45,
P=.001) was significantly associated with level of knowledge
of breast cancer. The variable of family income (x2=8.3,
P=.016) was significantly associated with breast self-examination
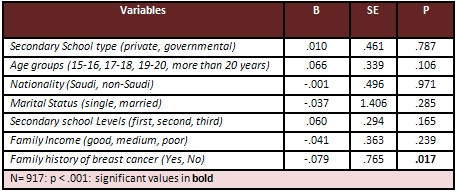
practice. Logistic regression analysis revealed that one of
seven predictors was significantly predictive of level of
knowledge scores; this was family history of breast cancer,
(b = - 0.079 , p < 0.05); the
negative of family history indicated that higher scores on
family history (e.g., no history of breast cancer) predicted
lower scores on the level of knowledge Table 5.
Table 5: Linear Regression Model of Demographic Variables
and Level of Knowledge
One of seven predictors were significantly predictive of performance
of self-examination scores; these included age groups; (B
= 0.33, p < 0.05) the higher scores on age group (e.g.,
20 yrs. or more) predicted higher scores on the performance
of breast self-exam ( e.g., Yes I perform breast self-exam)
Table 6.
Click here for Table
6 :Binary Logistic Regression Model for Performance of Breast
Self-Exam with Demographic Variables
Discussion
A study conducted in Saudi Arabia by Ibrahim et al estimated
that the future burden of breast cancer in Saudi Arabia is
expected to increase by approximately 350% by 2025(13).
The results of the study show that students had low knowledge
score in relation to breast self-examination; this reflects
the needs for targeting educational programs for female secondary
schools. This finding was consistent with several studies
in Saudi Arabia and in Malaysia (16,17) .
Concerning the risk factors about breast cancer, the present
study showed that most of the students had low knowledge of
breast cancer risk factors. The most widely known risk factors
by the students was smoking 49.4% followed by repeated exposure
to radiation on the breast (41.9%). This finding is similar
to that reported in Saudi Arabia (18) but most subjects didn't
know the association between breast cancer and age, using
oral contraceptive pills, avoiding breast feeding, obesity
and increased fatty food intake, previous history in the family.
However some studies have shown that the incidence of breast
cancer is said to be slightly higher in persons that have
a first degree relative with a history of breast cancer, persons
that have early menarche and late menopause, those that use
oral contraceptives, persons who do not breast feed and those
women having their first birth after age 35 or in nulliparous
women, the incidence is also increased with increasing age
of the patient, smoking, obesity, physical inactivity, radiation
exposure, intake of alcohol and high fat diet (16,19,20, 21
). These breast cancer risk factors can be changed with health
education. So health care professionals can play an important
role in educating students, to enhance their awareness of
breast cancer risk factors and influence their behavior. Slightly
more than half of the samples (52.2%) did not know the cause
of breast cancer. Similar results have been reported in previous
studies (19,22).
Regarding to the symptoms of breast cancer, most of the respondents
in this study did not know other warning signs of breast cancer
such as bloody discharge from nipple (49.6%), dimpling or
wrinkling in the skin of the breast (57%) and inverted nipple
(71.4%). This observation was also reported in other studies
(21,23 ). This reflects their lack of knowledge regarding
early symptoms of the disease, which is very important from
the point of view of better prognosis.
Concerning the screening methods for detecting the disease,
the participants in this study did not know about the use
of mammography and magnetic resonance imaging (MRI) as a screening
tool for early detection of breast cancer. This finding has
also been documented in previous studies (14,19,24,25 )MRI(16).
Health education about the benefits of mammography screening
for detection of breast cancer should be encouraged. Therefore
maternity nurses she have great influence on female students
to develop positive perceptions of breast cancer and motivation
to practice screening methods for early detection of the disease.
Regarding treatment, the respondents knowledge about the treatment
options of breast cancer showed that some of the respondents
were aware of treatment modalities of breast cancer the majority
of the respondent 52.1%, 48.4% knew that surgery and chemotherapy
respectively are the treatment options of breast cancer. This
result is similar to a study done by (Tiengo J.2011, Ibrahim
N .2009 )(21,26 ).
Regarding knowledge of practice of breast self-examination,
in this study about 2.3% of the students who heard about BSE
reported having performed it. From this only 3.4% performed
BSE monthly and the majority of the students performed BSE
irregularly (16.9%). Students knowledge about BSE might have
affected their monthly BSE performance. However, only a small
number of students who had knowledge about the BSE procedure
were performing BSE monthly. This may be due to insufficiency
of education programs organized to increase breast health
awareness. In this study, the findings regarding regular BSE
are different from a previous study done in Turkey which showed
that 20% of the students reported that they performed BSE
irregularly and only 6.7% of those who practice BSE performed
it regularly every month(27 ). The study done in Kuwait revealed
that only 14.0% perform BSE irregularly and only 7.1 % of
participants perform BSE monthly(19). In other studies the
percentage of monthly BSE performance has been found to be
3.4% among teenagers(28). This observation was also reported
in other studies (19,29).
A significant association was seen between family history
of breast cancer and overall level of breast cancer knowledge.
This finding was relatively consistent with findings in previous
research studies (24,30 ), while two studies showed a relation
between family history of breast cancer and regular BSE performance
(27,29). Another three studies revealed no relation between
family history of breast cancer and BSE performance (18,31,32
). This finding was consistent with conclusions drawn in earlier
studies, which found known breast cancer family history influenced
women's attitudes about breast cancer and their willingness
to engage in breast cancer screening behaviors (33). A negative
family history was found to be a significant lower predictor
on the level of breast cancer knowledge. But this result is
in contraindication with the findings of some other studies
that have found a positive family history of breast cancer
tends to show better awareness and functions and affected
women do more regular breast screening compared with the other
women (34,35).
Family income in this result was not significantly associated
with level of breast cancer, however family income was significantly
associated with BSE practice. In similar studies by (Alsaif
A ,2004 ; Dundar E ,2006)(31,36) showed no significant association
between family income with level of breast cancerknowledge
and BSE practice, unlike the findings of the present study
withfindings of a previous study by (Dandash K,2007) which
found a significant
relation between family income with level of breast cancer
knowledge and BSE practice (18).
Linear regression analysis reveals age group was significantly
predictive of performance of self-examination. The findings
of this study are consistent with those of other studies,
as many studies have found age was the most important predictor
for BSE practice (37,38,39). The findings of the present study
are contrary to the findings of some studies which found that
marital status, level of education, positive family history
of breast cancer, menarche and menopausal status were predictors
for BSE performance (34,37,38).
Conclusion
It is concluded that most of the female secondary school students
in Riyadh, Saudi Arabia had very low knowledge about breast
cancer. Recommendations are suggested to raise students' level
of knowledge toward breast cancer and practice of breast self-examination
among female students through the following activities; Developing
a health education programme that should be built into school
curricula, regarding breast cancer and BSE practice starting
from their secondary school. Developing educational programmes
for teachers. School health unit, mass media and Ministry
of Health should plan to raise awareness about breast cancer
in the community.
References
1- Glanz, K., Rimer, B & Lewis F. (2002). Health Behavior
and Health Education, 3rd ed. San Francisco: Jossey-Bass.
2- Gaballah I.(2011). Awareness, Knowledge and Practice of
Breast Self-Examination Among Saudi Women. Med. J. Cairo Univ;
79(2): 81 86. Available at : www.medicaljournalofcairouniversity.com
3- Beydag K, Karaoglan H. (2007). Effect of Training for self
breast examination on Knowledge and Attitude to University
Student. Preventive Medicine Bulletin of Turkish Armed Forces;6:106-111.
4- Jeber E, Soyer M, Ciceklioglu M&Climat S. (2006). Breast
cancer risk assessment and risk perception on nurses and midwives
in Bornova Health District in Turkey. Cancer Nurs; 29:224-249.
5- Esam Murshidy 19 June 2009, 1-37. Available at: http://www.oncology.org.sa
6- Ogletree R, Hamming B, Drolet J& Birch D.(2004). Knowledge
and intentions of ninth - grade girls after a breast self
examination program. Sch Health J ;74:365-369.
7- Rashidi A, Rajarom S. (2000). Middle Eastern Asian Islamic
Woman and breast self -examination. Cancer Nurs ; 23:64-70.
8- Gürsoy A, Y?lmaz F, Bulut H, Mumcu H, Ye?ilçiçek
K, Kahriman I& Hindistan S. (2009). The effect of peer
education on university students knowledge of breast self
examination and health beliefs. The Journal of Breast Health
; 5 (3 ).
9- Ogletree J, Hammig B, Drolet C & Birch A.(2004). Knowledge
and intentions of ninth-grade girls after a breast self-examinations
program. Journal of School Health; 74(9): 365-369.
10- American Cancer Society .Breast Cancer Facts &Figures
(2006-2007).
11- Baig S &Ali S.(2006). Evaluation of efficacy of self-breast
examination for breast cancer prevention: a cost effective
screening tool. Asian Pac J Cancer Prev ; 7(1): 154- 156.
12- Yarbro H.(2003). International nursing and breast cancer.
Breast J; 9( 2): 98- 100.
13- Yousuf S.(2010). Breast Cancer Awareness among Saudi Nursing
Students. Med. Sci.; 17 (3): 67-78 .
14- Maurer F. (1997). A peer education model for teaching
breast self-examination to undergraduate college woman. Cancer
Nurs; 20:49-61.
15- American Cancer Society: Cancer facts and figure 2009).
Available at: http:// www.cancer.org
16- Habib F, Salman S, Safwat M& Shalaby S .(2010). Awareness
and Knowledge of Breast Cancer Among University Students in
Al Madina Al Munawara Region. Middle East Journal of Cancer
; 1(4): 159-166.
17- Zavare M ,Joni M& Manaf R .( 2011). Knowledge on breast
cancer and practice of breast self-examination among selected
female university students in Malaysia. Medical and Health
Science Journal, MHSJ; 7:49-56 . Available at :www.academicpublishingplatforms.com
.
18- Dandash K & Al- Mohaimeed A. Knowledge, Attitudes,
and Practices Surrounding Breast Cancer and Screening in Female
Teachers of Buraidah, Saudi Arabia. International Journal
of Health Sciences, Qassim University ; 1(1) (January 2007/Muharram
1428H).
19- Alharbi N, Alshammari M, Almutairi B, Makboul G &
El-Shazly M.(2012). Knowledge, awareness, and practices concerning
breast cancer among Kuwaiti female school teachers. Alexandria
Journal of Medicine ;48:75-82.
20- Vahabi M.(2010). Knowledge of Breast Cancer and Screening
Practices Among Iranian Immigrant Women in Toronto J Community
Health ;36:265-273.
21- Tiengo J & Peltzer K .(2011). Knowledge attitude and
practice of breast cancer examination among women attending
a health facility in Gaborone ,Botswana. Gender & Behaviour;
9(1).
22- Ertem G& Koçer A .(2009). Breast self-examination
among nurses and midwives in Odemis health district in Turkey.
Indian Journal of Cancer; 46 (3).
23- Sambanje M,&, Mafuvadze B .(2012). Breast cancer knowledge
and awareness among university students in Angola. Pan African
Medical Journal; 11:70 .This article is available online at:
http://www.panafricanmedjournal.com/content/article/11/70/full/
24- Charkazi A, Samimi A, Razzaghi K, Kouchaki G&Moodi
M. Adherence to recommended breast cancer screening in Iranian
Turkmen women : the role of knowledge and beliefs . ISRN Preventive
Medicine ,Volume 2013, Article ID 581027, 8 pages .available
at : http://dx.doi.org/10.5402/2013/581027
25- Olowokere A, Onibokun A & Oluwatosin A.(2012). Breast
cancer knowledge and screening practices among women in selected
rural communities of Nigeria. Journal of Public Health and
Epidemiology ;4(9): 238-245.
26- Ibrahim N& Odusanya O.(2009). Knowledge of risk factors,
beliefs and practices of female healthcare professionals towards
breast cancer in a tertiary institution in Lagos, Nigeria.
BMC Cancer; 9(76).
27- Karayurt O , Özmen D & Çetinkaya A .(2008).
Awareness of breast cancer risk factors and practice of breast
self examination among high school students in Turkey. BMC
Public Health ; 8:359 .Available at :http://www.biomedcentral.com/1471-2458/8/359.
28- Ludwick R & Gaczkowski S.(2001). Breast self- exams
by teenagers. Cancer Nurs; 24:315-319.
29- Al-Naggar R, Al-Naggar D, Bobryshev Y, Chen R& Assabri
A .(2011). Practice and Barriers Toward Breast Self Examination
Among Young Malaysian Women. Asian Pacific J Cancer Prev;12:
1173-1178.
30- Royse D. & Dignan M.(2009). Improving cancer knowledge
and screening awareness: test of a telephone interviewer intervention.
Journal of Cancer Education; 24: 315-318.
31- Alsaif A.(2004). Breast self-examination among Saudi female
nursing students in Saudi Arabia. Saudi Med J; 25 (11): 1574-1578.
32- Jirojwong S & MacLennan R.(2003). Health beliefs,
perceived self-efficacy, and breast self-examination among
Thai migrants in Brisbane. Journal of Advanced Nursing ;41:241-249.
33- Bird Y., Moraros J & Banegas P.(2010). Breast cancer
knowledge and early detection Among Hispanic women with a
family history of breast cancer along the U.S.- Mexico border.
Journal of Health Care for the Poor and Underserved; 21 (2):
475-488.
34- Hajian S, Vakilian K, Najabadi K, Hosseini J& Mirzaei
H.(2011). Effects of Education Based on the Health Belief
Model on Screening Behavior in High Risk Women for Breast
Cancer, Tehran, Iran. Asian Pacific J Cancer Prev; 12: 49-54.
35- Ceber E, Yücel U, Mermer G, et. al (2009). Health
beliefs and breast self-examination in a sample of Turkish
women academicians in a university. Asian Pac J Cancer Prev;
10, 213-8.
36-Dündar E, Ozmen D, Ozturk B, Haspolat G, Akyildiz
F & Colan G. (2006). The knowledge and attitudes of breast
self-examination and mammography in a group of women in a
rural area in western Turkey. BMC Cancer; 6, 43.
37- Avci IA .(2008). Factors associated with breast self-examination
practices and beliefs in female workers at a Muslim community.
Eur J Oncol Nurs; 12: 127-133.
38- Noroozi A, Jomand T& Tahmasebi R.(2010). Determinants
of Breast Self-Examination Performance Among Iranian Women:
An Application of the Health Belief Model, J Canc Educ ,DOI
10.1007/s13187-010-0158-y
39- Parsa P, Kandiah M& Abdul Rahman H.(2006). Barriers
for Breast Cancer Screening Among Asian Women: A Mini Literature
Review. Asian Pacific J Cancer Prev;7: 509-514
40- American Cancer Society: Breast Cancer Fact and Figures.2008
http://www.cancer.org/downloads/STT/CAFF2005BrFacspdf2005pdf
|
 |

