| |
January
2015
- Volume 9, Issue 1
The
Use of Patient-Based Pain Education to Reduce Barriers to
Cancer Pain Management: A Literature Review

|
 ( (
|
Saleh Mahmoud Mayyas
Correspondence:
Saleh Mahmoud Mayyas,
RN, MSN
Madinah Cardiac Center
Saudi Arabia
Email: mayyassaleh@gmail.com
|
|
|
Abstract
Introduction: the treatment of cancer pain is
considered as a complicated process. Many cancer patients
with pain report that they are undertreated, despite
the utilization of best international guidelines for
treating cancer pain. Barriers to cancer pain management
are thought to have a contributory role in the undertreatment
of pain. Educational programs have focused on treating
barriers to pain management in patients with cancer.
Purpose: to evaluate the efficacy of pain education
programs in reducing barriers to cancer pain management.
Methodology: using the key words pain education program,
cancer patients, barriers, and pain management; an electronic
search was conducted on the databases Pubmed, Google,
and Science Direct. The end result of the search led
to selection of ten articles to build the evidence for
use in clinical practice.
Findings: all of the articles used in this review
indicated that pain education can reduce barriers to
cancer pain management.
Conclusion and Recommendations: pain education
programs are an effective approach in the treatment
of patient-related barriers to cancer pain management.
It is strongly recommended to integrate PEP within the
treatment course of cancer pain. Further, it is reinforced
that all institutions dealing with cancer patients hold
specialized health care professionals who are able to
administer PEPs.
Key words: pain education program, cancer patients,
barriers, pain management
|
Introduction
Pain is one of the most distressing symptoms affecting patients
with cancer at different stages of the disease. Nevertheless,
it is estimated that one of two cancer patients with pain
do not receive effective management for their pain, despite
international guidelines that aim to treat cancer pain including
the World Health Organization (WHO) and the National Cancer
Institute (NCI) guidelines.[1-3].
Barriers to cancer pain management include patient related
barriers, health care professional barriers, and system barriers;
usually lead to the undertreatment of pain.[4]. Patient related
barriers include misconceptions about analgesics and their
side effects, nonadherence to treatment regimens, and poor
pain communication with health care providers[5]. As a definitive
approach to reduce patient related barriers to cancer related
management Pain education program (PEP) has evolved. PEP includes
comprehensive information regarding pain and pain treatment
including the definition and causes of pain, pain treatment
approaches and their side-effects, myths and misconceptions
about pain management, consequences of mal-adherence to prescribed
treatment, the use of nonpharmacologic pain treatment, and
pain assessment.[6]. Thus, this review aims to evaluate whether
pain education programs can reduce patient barriers to pain
management in adult cancer patients or not.
PICO
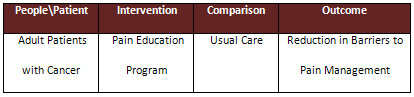
PICO Question
What is the effect of a pain education program on barriers
to pain management in adult patients with cancer?
Methodology
Electronic literature search using the key words: pain education
program, cancer patients, barriers, and pain management was
done seeking articles published between the years 2008 and
2013 on the databases Pubmed, Google, and Science Direct.
A total of 109 articles have been retrieved. After selection
based on the abstract and contents of the articles, ten articles
were selected to build the evidence for evaluating the effect
of pain education programs on barriers to cancer pain management
as a general term or on specific aspects of those barriers.
Nine of these articles are randomized controlled trials which
are level two of evidence. The remaining article is a quasi-experimental
article that is classified as level three of evidence.
Findings
A randomized, controlled study; that included 176 subjects,
assessed the effect of representational intervention on decreasing
barriers to pain management in patients with cancer. The study
is determined as level two of evidence. The representational
program adopts that a change (can be inferred to be a reduction
in barriers to cancer pain management) is facilitated when
individuals are given the opportunity to monitor and comment
on their own ideas, whereas this can be achieved by education.
The subjects in the representational programs reported less
barriers score than those in the control group[7]. In another
randomized controlled study (level two evidence), Ward and
colleagues evaluated the efficacy of a tailored educational
intervention in reducing attitudinal barriers held by patients
with cancer. After the intervention, the group received educational
intervention has shown significantly lower attitudinal barriers
scores compared to the two other groups[8]. In Turkey, a randomized
controlled design (level two of evidence) was used to investigate
the effect of pain education program on pain intensity, pain
treatment satisfaction, and barriers in patients with cancer.
The study concluded that PEP results in decreased barriers
scores in patients with cancer.[5] Aiming to test the effect
of an educational program combined with system change interventions
on reducing barriers to pain and fatigue management, a quasi-experimental
study (level three of evidence) was conducted. In this study,
the intervention was found to be effective in reducing barriers
to pain management in patients with cancer[9]. Even short
educational interventions were found to reduce barriers to
cancer pain management as evidenced by a randomized controlled
study (level two of evidence) conducted by Smith and colleagues[10].
Al-Atiyyat (2008) has summarized the barriers cancer patients
have toward pain management. Among these barriers, is the
belief that ''good'' patients do not complain about pain,
which consequently leads to underreporting of their pain.
Improving patient's communication of pain through educational
sessions in cancer patients holds the premises of overcoming
patient's negative misconceptions about analgesics, increasing
adherence to pain medications, and achieving effective pain
management in those patients[11,12]. In order to investigate
the effectiveness of tailored education and coaching intervention
on pain outcomes, a randomized controlled study (level two
of evidence) that included 258 patients was conducted. Among
these outcomes is pain communication self-efficacy that is
found to improve significantly after receiving the intervention[4].
In order to enhance patient communication of cancer pain to
physicians, an experimental study was conducted. The intervention
group received Tailored Education Coaching (TEC) intervention
that helps patients learn pain management and communication
skills. After the intervention, patients in the TEC group
were more able to discuss their pain concerns with their physicians
than those in the control group[13].
Lack of knowledge about pain and pain treatment leads to negative
attitudes toward complying with pain treatment.[14]. Therefore,
improving patient's knowledge about pain will enhance the
outcome of pain management. In a randomized controlled study
that is determined as level two of evidence, 120 patients
were randomized to PEP and control groups. The knowledge of
pain improved significantly after receiving PEP[15].
Adherence to analgesic use serves as an indicator to which
degree patients are holding barriers to pain management. Oldenmenger
and her colleagues conducted a randomized controlled study
that is level two of evidence. The aim of the study was to
assess the effect of Pain Education Program and Pain Consultation
(PEP-PC) on pain levels, pain interference, and adherence
to analgesic use. The PEP-PC was found to improve adherence
to analgesic use[5].
A a study conducted by Lovell and colleagues evaluated the
effect of an intervention that affords booklet and videos
about pain and pain management on improving pain outcomes
in patients with cancer. Using a randomized, controlled design,
which is determined as level two of evidence, the intervention
resulted in decreased pain intensity and in the reduction
of the addiction subscale score of the barriers questionnaire[16].
Appraisal of the Evidence
Strengths of the Evidence
Among the strength points of this evidence is that most of
the articles included are level two of evidence, with the
exception of one article that is level three of evidence.
Another strength point is that all of the references used
in the evidence were conducted within the years 2008 till
2013. The references in this evidence were selected from international
journals, without the need to revise internet websites, posing
additional strength for the evidence.
Limitations of the Evidence
Two of the articles had low sample sizes of 40 and 42 patients;
however, the sample size in the other studies enhances the
generalizability of the evidence. One of the limitations of
this evidence is that the barriers questionnaire used along
all of the articles was not the same version which may affect
the consistency of the findings in this evidence.
Summary of the Evidence
Among the ten articles considered to be used in this paper,
six articles focused on assessing the effectiveness of educational
interventions on reducing barriers to cancer pain management.
The articles have found that education can be an effective
approach to reduce barriers to pain management in patients
with cancer. One of the articles evaluated the efficacy of
PEP in improving cancer patient's knowledge about pain, and
found that PEP is an effective approach to improve patient's
knowledge about pain. Two of the articles assessed the effect
of PEP on cancer patient's pain communication. PEP was found
to improve pain communication efficacy in patients with cancer.
Another study proved that PEP improves patients' adherence
to analgesic use. One of the articles has investigated the
advantage of the use of self-administered PEP via booklet
and\or videotapes in the treatment of patient barriers to
cancer pain management; the intervention was effective in
reducing some of the barriers related to the fear of addiction.
Conclusion
Barriers to pain management are the leading cause of under
treatment of pain in patients with cancer. Based on the findings
of this evidence, it can be concluded that pain education
programs are an effective approach in the treatment of patient-related
barriers to cancer pain management. It is strongly recommended
to integrate PEP within treatment schedules planned for patients
with cancer. Focusing on the barriers each patient holds will
be more efficient than to provide them with information that
is already known to him\her. It is important to provide all
health care institutions with professionals who are able to
administer PEPs.
References
[1] van den Beuken-van Everdingen MH, de Rijke JM, Kessels
AG, Schouten HC, van Kleef
M, Patijn J. Prevalence of pain in patients with cancer: a
systematic review of the past 40
years. Annals of Oncology. 2007 Mar;18(9):1437-49.
[2] Deandrea S, Montanari M, Moja L, Apolone G. Prevalence
of undertreatment in cancer pain. A review of published literature.
Annals of oncology. 2008 Dec;19(12):1985-1991. doi: 10.1093/annonc/mdn419.
[3] Valeberg T.B., Tone R., Bjordal K., Hanestad R.B., Paul
S., Miaskowski C. Self-reported prevalence, etiology, and
characteristics of pain in oncology outpatients. European
Journal of Pain. 2008 July;12(5):582-90
[4] Kravitz, L.R., Tancredi J.D., Tim G. et al. Cancer Health
Empowerment for Living without Pain (Ca-HELP): Effects of
a tailored education and coaching intervention on pain and
impairment. Pain. 2011 July;152(7):1572-82. doi:10.1016/j.pain.2011.02.047
[5] Oldenmenger H.W., Smitt A.E.S.P., Cees V.A.G.M., de Raaf
J.P., van der Rijt C.C. A combined pain consultation and pain
education program decreases average and current pain and decreases
interference in daily life by pain in oncology outpatients:
A randomized controlled trial. Pain. 2011 Nov;152(11):2632-9
doi:10.1016/j.pain. 2011.08.009
[6] Yildirim, K.Y., Cicek F., Uyar M. Effects of Pain Education
Program on Pain Intensity, Pain Treatment Satisfaction, and
Barriers in Turkish Cancer Patients, Pain Management Nursing.
2009 Dec;10(4):220-8. doi: 10.1016/j.pmn.2007.09.004.
[7] Ward E.S., Donovan H., Gunnarsdottir S., Serlin C.R.,
Shapiro R.G., Hughes S. A Randomized Trial of a Representational
Intervention to Decrease Cancer Pain (RIDcancerPain). Health
Psychology.2008 Jan;27(1):59-67. doi: 10.1037/0278-6133.27.1.59.
[8] Ward E.S., Ko Kung Wang, Serlin S.R., Peterson L.S., Murray,
E.M. A randomized trial of a tailored barriers intervention
for Cancer Information Service (CIS) callers in pain. 2009
July;144(1):49-56. doi:10.1016/j.pain.2009.02.021
[9] Borneman T., Koczywas M., Sun V.C., Piper B.F., Uman G.,
Ferrell B. Reducing Patient Barriers to Pain and Fatigue Management.
Pain Symptom Management. 2010 Mar;39(3):486-01. doi:10.1016
[10] Smith Y.M, DuHamel N.K., Egert J., Winkil G. Impact of
a brief intervention on patient communication and barriers
to pain management: Results from a randomized controlled trial.
Patient Education and Counseling. 2010 Oct;81(1):79-86. doi:10.1016/j.pec.
2009.11.021
[11] Al-Atiyyat N.M.H., Patient-Related Barriers To Effective
Cancer Pain Management, Hospice and Palliative Nursing. 2008
Aug;10(4):198-04
[12] Aranda S, Yates P, Edwards H, Nash R, Skerman H, McCarthy
A. Barriers to effective cancer pain management: a survey
of Australian family caregivers. European Journal of Cancer
Care. 2004 Sep;13(4):336-43. doi: 10.1111/j.1365-2354.2004.00483.x
[13] Street J.L R., Slee C., Kalauokalani K.D., Dean E.D.E.,
Tancredi J.D., Kravitz, L.R. Improving physician-patient communication
about cancer pain with a tailored education-coaching intervention.
Patient Education and Counseling.
2010 Jul;80(1):42-7. doi: 10.1016/j.pec.2009.10.009
[14] Riddell A., Fitch M.I. Patients' knowledge of
and attitudes toward the management of
cancer pain. Oncology Nursing Forum. 1997 Nov-Dec;24(10):1775-84
[15] Van der Peet H.E., van den Beuken-van Everdingen H.J.M.,
Patijn J., Schouten C.H,
van Kleef M., Courtens M.A. Randomized clinical trial of an
intensive nursing-based pain
education program for cancer outpatients suffering from pain.
Support Care Cancer. 2009
Aug;17(8):1089-99. doi 10.1007/s00520-008-0564-4
[16] Lovell, R.M., Stockler R.M., Chye R., Goldstein D., &
Boyle M.F. A Randomized Controlled Trial of a Standardized
Educational Intervention for Patients with Cancer Pain. Pain
and Symptom Management. 2010 July;40(1):49-59, doi: 10.1016/j.jpainsymman.
2009.12.013
|
 |

