| |
February
2014
- Volume 8, Issue 1
Assessing the
perception of nurses about privacy of patients

|
 ((2) ((2)
|
Manal AL-Bitawi
Ahmad AL- Omari
Correspondence:
Manal AL-Bitawi RN
PO box. 36033 Alhashmy Aljanoubi Amman Jordan 11120
Email: manalbetawy@yahoo.com |
Introduction
Privacy is a legal right of
patient/client, which flows from the fundamental rights to
life, liberty and property, drives from the right to enjoy
life and to be left alone (1+7+8). Respect for patients' privacy
and dignity are long established principles of nursing practice
(10). Invasion of a patient's privacy decreases the quality
of care that is provided for the patient and decreases the
trust of the patient in the medical team, which has a negative
effect on the health status of the patient (2+4).
The concept of patient privacy is
used in many disciplines and is recognized as one of the important
concepts in nursing (3+10). In the practice, there are many
forms for the patient privacy, including the physical, informational,
decisional and proprietary privacy (5). In fact, even though
most healthcare professionals know the limits of patient privacy
and its forms very well, they have trouble applying them to
their behaviors, particularly in hospital lifts where discussions
of patients' information may be overheard, or when the patient's
body parts need to be exposed (6+9). This gap between the
privacy perception and the privacy practice directs us toward
this study. The purpose of this study is to assess the current
practices and problems that are encountered with the perception
of patient privacy among registered nurses at King Hussein
Hospital.
Methodology
Descriptive design was used for this study. A convenience
sample of 100 registered nurses was selected from both genders
with different experiences, who are working in surgical and
medical floors, in addition to critical units at King Hussein
Hospital (Table 1).
Table 1: The characteristics of the sample
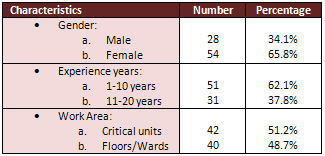
A questionnaire was developed by the researchers and consisted
of 20 statements that assessed mainly physical and informational
privacy. The four point Likert scale questionnaire was reviewed
by an expert panel consisting of nurse educator, nurse administrator
and senior nurse colleague to establish its content validity.
The stability reliability was checked by administering the
questionnaire to a group of 30 registered nurses selected
conveniently from both genders with different experiences.
Then after 2 weeks, the same instrument was administered to
the same group. The correlation coefficients were calculated,
and it was equal to (+0.80).
The Data collection was carried out
on 14th of January 2010. Response rate was 82% (n=82).
Results
The patient privacy in our study was divided into two main
divisions: Physical privacy and Informational privacy. Physical
privacy includes preparing the environment that ensures patient
privacy before any procedure is provided to the patient, like
closing the room door or the drape, dismissing the visitors
and company. Physical privacy also includes obtaining patient
permission to expose any part of his/her body during any procedure.
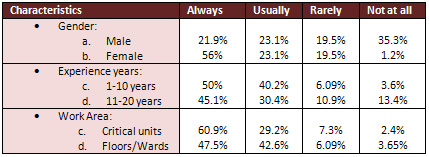
In our study, 55.5% of the nurses were always protecting the
physical privacy, 34.9% usually, 7.4% rarely and 1.8% not
at all. (Table 2)
Table 2: The protecting of patients' physical Privacy
The other type of patient privacy
in our study was informational privacy, which includes protecting
all the information and records concerning patients, and not
sharing this information or records with anyone outside the
patient's medical team without the patient's permission. In
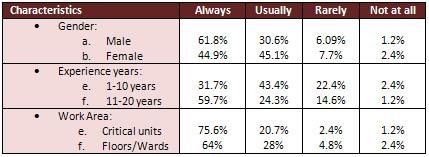
our study, just 18.5% of the study nurses were always protecting
the informational privacy, 21.9% usually, 26.5% rarely and
32.8% not at all (Table 3).
Table 3: The protecting of patients' informational Privacy
On the other hand, 53.6% of the study
nurses think that the most common invasions of the patients
privacy is caused by the visitors and patient's company. While
36.5% of the study nurses think that the most common invasions
of patient's privacy were caused by the health team members
themselves.
Discussion
Physical and informational privacy are the most well known
types of patient privacy among nurses (5). In the empirical
studies, the concept of privacy has mainly been studied in
hospital organizations using the physical dimension (5).
In our study, physical privacy was protected always &
usually by 90% of the participants, which reflects the high
standardized care that is provided by nurses. On the other
hand, the results show that female nurses protect physical
privacy more than male nurses, while the less experienced
nurses (1-10 years) protect the privacy more than the highly
experienced nurses (11-20 years). The less experienced nurses
are more restricted by the rules of the hospital. The work
area also has its effect on the physical privacy; in critical
units where there is a highly qualified team and more restriction
on the visitors, physical privacy is more protected (~80%)
than the floors.
The other type of privacy in our study is informational. Just
40.4% of the nurses were always and usually protect informational
privacy. This small percentage in comparison with the physical
privacy reflects the high need to train the nurses about how
to protect informational privacy. Gender also had its effect
on informational privacy; we find that the male nurses more
protect the informational privacy than females. In addition,
in the critical units informational privacy is also more protected
than on the floors. The previous studies found that informational
privacy was poorly protected in floors (10).
The causes for invasion of privacy in our study were the visitors
mainly, then by the medical team. In the previous studies,
the causes were mainly by the medical team not by the visitors
(4+6+10).
Conclusion
and Recommendations
An assurance of patient's privacy is necessary to secure effective,
high quality health care. Breaches of a patient's privacy
compromises ethical health care and undermines patients' confidence
in caregivers. Healthcare institutions must provide effective
training to minimize these breaches. We hope that the Royal
Medical Services will heed the call to improve discretion
for the patients who entrust us with their care.
References
1. Smeltzer, S., & Bare, B. (2003). Brunner and Suddarth's
textbook of medical-surgical nursing (10th edition). Philadelphia:
Lippincott. Chapter 3.pages (30-33).
2. Kozier, B., & Erb, G. (2004). Fundamentals of nursing
(7th edition). New Jersey: Pearson Education. Chapter 4. Pages
(58-61).
3. Bickley, L. S.,& Hoekelman, R. A (1999). Bates' guide
to physical examination and history taking (7th ed.). Philadelphia:
Lippincott Williams & Wilkins.
4. Day, L. J. , & Standard, D. (2006). Developing trust
and connection with patients and their families. Critical
Care Nurse, 19(3), 66-70.
5. Leino-Kilpi, H. Välimäki, T. Dassen, M. Gasull,
C. Lemonidou, A. Scott, M. Privacy: a review of the literature.
International Journal of Nursing Studies, Volume 38, Issue
6, December 2001, Pages 663-671.
6. Vigod, S. & Bell, C. Privacy of patients' information
in hospital lifts: observational study. BMJ 2003, 327; 1024-1025.
Available from: http://www.bmj.com/search/patientprivacy.html
7. American Nurses Association.(2009). Code of ethics for
nurses with interpretive statements. Washington, DC: American
Nurses Publishing.
8. Jordanian Nursing Council (2009). Code of ethics for nurse's
practice. Amman: Jordanian Nursing Council Publishing.
9. Haddad, A. (2001). Ethics in action. RN, 64(1), 29-30,32.
10. Rylance, G. Privacy, dignity, and confidentiality: interview
study with structured questionnaire. BMJ 2001, 318;301-303.
Available from: http://www.bmj.com/search/patientprivacy.html
|
 |

