| |
April
2014
- Volume 8, Issue 2
A survey of
nurses' perceived barriers to research utilization in Bahrain
in comparison to other countries

|
 ( (
|
Nawal Buhaid
Rosalind Lau
Margaret O'Connor
Correspondence:
Dr. Rosalind Lau
Research Fellow
School of Nursing & Midwifery
Monash University, Clayton Campus
Wellington Rd
Clayton, Victoria 3800
Australia
Phone: +61-3 9902 0552
Fax: +61-3 9905 4837
Email:
rosalind.lau@monash.edu
|
|
|
Abstract
Background: Nurses play a vital role in using
the best available research evidence to provide optimal
care for patients. Despite the importance of nurses'
uptake of research utilization, little is known about
the uptake of research utilization among nurses in Bahrain.
Objectives: This study investigated the perceived
barriers to research utilization in Bahrain and compared
the barriers to those of other countries.
Methods: This is a cross-sectional exploratory
study carried out among the registered nurses in a major
teaching and research hospital in Bahrain. The Barriers
to Research Utilization Scale (Barriers Scale) was used
to collect the data.
Results: The results showed that the top three
ranked perceived barriers were lack of authority to
change practice, inadequate facilities and time constraints.
Of the top 10 ranked perceived barriers, six items were
related to the subscale 'organization' (the setting)
and four to the subscale 'presentation' (report and
accessibility of research findings).
Conclusions: If research utilization is to be
enhanced in Bahrain, the local organizational barriers
need to be addressed. An important step is to create
an organizational environment that recognizes the value
of research and encourages and supports nurses' research
activities.
Key words: Bahrain, barriers, Barriers Scale,
evidence-based practice, research utilization
|
Introduction
Over the past two decades,
nurse leaders have attempted to address the issue surrounding
the utilization of research in practice. They have emphasized
the use of scientific evidence-based research to improve patients'
quality of care.(1) Swan et al(2) argued that nurses need
to implement the best available evidence to optimize patient
care and meet the challenges facing health services. Despite
increasing efforts by nurse leaders to promote the utilization
of research in nursing practice, it is still a challenge and
the uptake is slow. It has been postulated that this persistent
gap is due to a range of barriers that hinder the nurses in
implementing evidence-based clinical practice. To bridge the
gap between what is known and what transpires in practice,
a common approach is to identify barriers for changing practice.
Barriers to research utilization
have been extensively explored in Western countries including
the United States (USA),(3, 4) United Kingdom (UK),(5-7) and
Scandinavia.(8, 9) The relevance and applicability of these
findings to nursing practice in Bahrain must be considered
cautiously, because the health care system and professional
culture from Bahrain is different from these countries.
Only recently studies have explored
research utilization among the nurses in the Middle East where
the culture and delivery of health care, including nursing,
are significantly different from Western countries. A Turkish
study found the lack of time to implement new ideas was the
most frequently perceived barrier. Another two Turkish studies
found the main barrier was inadequacy of facilities to implement
research.(10, 11) An Iranian study found barriers to research
utilization were time constraints, inadequate facilities and
lack of autonomy of nurses to change nursing practice.(12)
Another Iranian study found that in general, nurses held positive
attitudes toward research; however, the majority of nurses
were not convinced of the importance of research to nursing
practice and to the nursing profession.(13)
To our knowledge, no study has investigated
Bahraini nurses' perceptions of barriers to research utilization
and this study was conducted to fill that gap. The aims of
this study were to identify perceived barriers to research
utilization in Bahrain and to compare the barriers to those
of other countries.
Methods
This is a cross-sectional exploratory research design. A convenience
sample of registered nurses was recruited from a large tertiary
government hospital in Bahrain which functions as the center
of teaching and research for health professionals. This hospital
has 54 wards and 946 beds. At the time of the survey, the
total number of nurses in Bahrain was estimated to be 3,037,
of which 256 were males and 2,781 were females.(14)
The inclusion criteria for the study
were: registered nurses, more than one year of nursing experience,
and aged 20 years or over. Exclusion criteria were: student
nurses and practical-trained workers with no nursing degree.
Procedure
Data were collected during December 2008. Six weeks before
the commencement of the survey, a set of questionnaires, an
explanatory statement and the approval letter from the Ministry
of Health, Kingdom of Bahrain were sent electronically to
the Chief of Nursing Services of the hospital to seek permission
to conduct the study. After permission was granted, two weeks
before the commencement of the study, a flyer and the invitation
to participate in the study was sent to the nursing administration
to be distributed to the wards. In addition all head nurses
and ward supervisors in nursing administration were informed
of the study.
The researcher delivered the questionnaires
to the ward supervisors or acting senior nurses who then distributed
them to the nurses. The participants were asked to return
the completed questionnaire in a sealed envelope to their
ward supervisors, or to the boxes placed in the nursing administration
area. All responses were anonymous. One week after the distribution
of the questionnaire an electronic mail was sent to the wards
to remind those nurses who had not completed the questionnaire,
followed by a second reminder one week later. In addition,
the researcher regularly visited the clinical areas to answer
questions and was in constant contact by phone with supervisors
to track the number of returned questionnaires.
Instrument
The data was collected using the Barriers to Research Utilization
Scale (Barriers Scale) which is the most widely used standard
of measurement for the nurses. The Barriers Scale was originally
developed in the USA in the 1980s and modified by Funk et
al.(3) The theoretical foundation for the development of the
Barriers Scale was Rogers' diffusion of Innovations theory.(15)
Diffusion theory is the process by which an innovation is
communicated through particular channels over time among the
members of a social system. The Barriers Scale consists of
four subscales: (1) 'nurse' refers to the individual nurse's
research values, skills and awareness; (2) 'organization'
refers to the barriers and limitations imposed by the setting;
(3) 'research' refers to the characteristics and quality of
study evidence; and (4) the 'presentation' refers to the report
and accessibility of research findings.
The Barriers Scale asks participants
to rate on a five-point Likert scale the extent to which they
consider each of the 29 items as a barrier to research utilization.
The response options range from 1 to 5 with 1: to no extent,
2: to a little extent, 3: to a moderate extent, 4: to a great
extent, 5: no opinion. The factor analysis found the item:
'the amount of research information is overwhelming' failed
to load on any factor, but was retained based on the feedback
from clinicians and administrators.(3) A high mean score signifies
a greater barrier. Most studies that used the Barriers Scale
presented their findings in rank order, based on the percentage
of participants agreeing with each item being a moderate or
great barrier to research utilization.
The reported internal consistency
reliability of the instrument was modest.(3) The Cronbach's
alpha of each subscale was: nurse = 0.80; organization = 0.80;
research = 0.72; and presentation = 0.65. To determine the
internal consistency of the instrument on this sample, Cronbach's
alpha coefficient was performed. The Cronbach's alpha for
this study ranged from 0.63 to 0.78, which was lower than
that reported by Funk et al.(3)
Ethical considerations
Approval to conduct the study was sought and granted by an
Australian University Human Ethics Committee where the third
author was studying, as well as the research technical support
team from the Ministry of Health, Kingdom of Bahrain.
Data analysis
The analyses were performed using the SPSS Version 17 (SPSS
Inc., Chicago, IL, USA). The results were presented using
descriptive statistics (counts, percentages, means and standard
deviations). The response options "to a great extent"
and "to a moderate extent" were merged into one
category.
Results
Participant characteristics
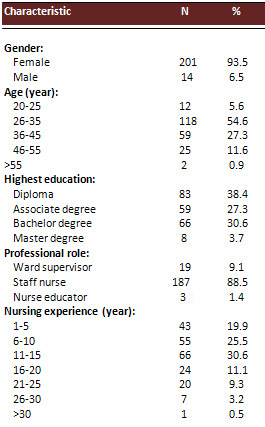
A total of 250 questionnaires were distributed and 219 were
returned, giving a response rate of 87.6%. Two hundred and
one (93.5%) female nurses and 14 (6.5%) male nurses participated
in the study. The majority of the participants were staff
nurses (88.5%), followed by ward supervisors (9.1%). The majority
of nurses (87.6%) were in the age group 20-45 years. The average
age for the participants was 35 years. Eighty three (38.4%)
of nurses held a Diploma degree and sixty six (30.6%) held
a Bachelor degree. Sixty six nurses (30.6%) had 11-15 years
of nursing experience and the average was 12 years. Details
of the demographic characteristics are presented in Table
1.
Table 1: Demographic profile of the participants
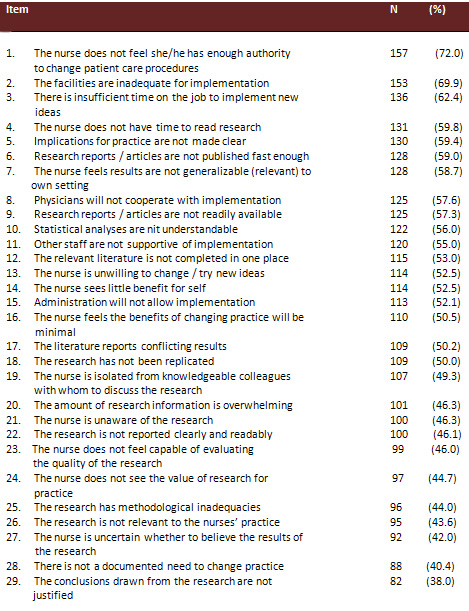
Perceived barriers to research
utilization
When "moderate" and "great extent" of
the barriers were combined and analyzed, the top three perceived
individual items were related to the subscale organization,
'the nurse does not feel she/he has enough authority to change
patient care procedures' (72%); followed by 'the facilities
are inadequate for implementation' (69.9%); and 'there is
insufficient time on the job to implement new ideas' (62.4%).
Of the lowest three ranked items, two were related to the
subscale research and one to the subscale nurse. The three
lowest ranked items were 'the conclusions drawn from the research
are not justified' (38%); 'there is not a documented need
to change practice' (40.4%) and 'the nurse is uncertain whether
to believe the results of the research' (42.0%).
Of the top 10 items perceived as
a barrier, six were related to the subscale organization and
four to the subscale presentation. Of the least 10 items perceived
as a barrier, four were related to the subscale nurse, three
to the subscale research, two to the subscale presentation
and one individual item which was not included in any of the
subscales: 'the amount of research information is overwhelming'.
The ranked order of the perceived barriers to research utilization
is presented in Table 2.
Table 2: Rank order of barriers to research utilization
In terms of the subscale, the highest
barrier was organization and the least barrier was research.
The mean values and the standard deviation for each of the
subscales were as follows: organization (2.78, SD 0.64), presentation
(2.73, SD 0.58), nurse (2.58, SD 0.61), and research (2.53,
SD 0.49).
Comparison between Bahrain and
other countries
To date, there have been a significant number of studies conducted
on research utilization among nurses worldwide using the Barriers
Scale. In the selection of the studies for comparison, we
decided on those who used the Barriers Scale in the last five
years; these are presented in Table 3. Regardless of the country,
the greatest barrier was related to the subscale organization,
however there were differences on the individual items within
the subscale.
Table 3: Comparison of studies using Barriers Scale in
the last 5 years
|
Author
|
Sample
|
Greatest
barrier
|
Second
greatest
barrier
|
Third
greatest barrier
|
|
This study
|
This study Bahrain
N = 219
Mixed setting
Clinical nurses = 187
Supervisors = 19
Nurse educators = 3
|
The nurse does
not feel she/he has enough authority to change patient
care procedures
|
The facilities
are inadequate for implementation'
|
There is insufficient
time on the job to implement new ideas
|
|
Aktinson et
al. 2008
|
USA
N = 249
Community
Clinical nurses = 213
The role of 36 participants not reported
|
The nurse does
not feel she or he has enough authority to change patient
care procedures
|
There is insufficient
time on the job to implement new ideas
|
Nurse does not
has time to read research
|
|
Boström
et al. 2008
|
Sweden
Community aged care
Clinical nurses = 140
|
The nurse is
isolated from knowledgeable colleagues with whom to
discuss the research
|
The facilities
are inadequate for implementation
|
The relevant
literature is not compiled in one place
|
|
Chau et al.
2008
|
Hong Kong
Mixed setting
Clinical nurses = 1,156
Nursing officers = 166
Ward/Department Operational managers = 36
Nurse specialists = 29
Advanced practice nurses = 40
Others = 31
|
The facilities
are inadequate for implementation
|
Lack of authority
to change practice
|
Lack of time
to implement new ideas
|
|
Mehrdad et al.
2008b
|
Iran
Mixed setting
Clinical nurses = 316
Head nurses = 59
Nurse educators = 35
|
The nurse does
not have time to read research
|
Facilities are
inadequate for
implementation
|
Nurses do not
feel they have
enough authority to change patient
care procedures
|
|
Kocaman et al.
2009
|
Turkey
Mixed setting
Clinical nurses = 329
|
There is insufficient
time on the job to implement new ideas
|
Research reports/article
are written in English
|
The facilities
are inadequate for implementation
|
|
Yava et al.
2009
|
Turkey
Medical/surgical wards
Clinical nurses = 549
Nurse managers = 74
Nurse educators = 8
|
The nurse does
not feel she / he has enough authority to change patient
care procedures
|
The nurse does
not have time to read research
|
The facilities
are inadequate for implementation
|
|
Brown et al.
2010
|
USA
Mixed setting
Clinical nurses = 226
Nurse managers = 107
CNS/Nurse educator s = 48
NPs/Midwifes = 105
|
The nurse does
not have time to read research
|
There is insufficient
time on the job to implement new ideas
|
The nurse does
not have authority to change patient care
|
|
Chien 2010
|
Hong Kong
Mixed setting
Clinical nurses = 550
|
The nurse does
not feel she has enough authority to change patient
care procedures
|
There is insufficient
time on the job to implement new ideas
|
The nurse does
not feel capable of evaluating the quality of research
|
|
Uysal et al.
2010
|
Turkey
Medical/surgical wards
Clinical nurses = 216
|
The facilities
are inadequate for
implementation
|
The relevant
literature is not compiled in one place.
|
Physicians will
not cooperate with implementation
|
|
Sari et al.
2012
|
Turkey
Mixed setting
Clinical nurses = 622
Head nurses/ supervisors/ directors = 96
|
The facilities
are inadequate for implementation
|
The relevant
literature is not compiled in one place.
|
The nurse is
unaware of the research
|
Of the ten studies; three studies,
one from USA,(16) one from Hong Kong,(17) and one from Turkey(11)
reported 'the lack of authority to change patient care procedures'
as the greatest barrier to research utilization. This individual
item was reported in the top three of all the studies, except
for a more recent study conducted in Turkey where it was ranked
nine.(18) Three studies; one from Hong Kong(19) and two from
Turkey(10, 18) reported 'inadequate facilities for implementation'
as their greatest barrier. Three studies; one from USA,(20)
one from Turkey(21) and one from Iran(12) reported time constraints
as the greatest barrier. One Swedish study reported feeling
isolated from experienced colleagues to discuss research as
the greatest barrier.(22)
Discussion
In this study, the highest subscale barrier was 'organization'.
This was a surprising finding given that the study was conducted
in a hospital which functions as the center of teaching and
research for health professionals. One would expect the institution
to support the nurses in using research evidence in their
practice. Nevertheless the finding supports the integrative
review on the Barriers Scale undertaken by Carlson et al,(23)
who commented that studies using Barriers Scale have a high
degree of consistency, suggesting that barriers to research
utilization by nurses have not changed.
The ranking of each item in this
study has shown considerable consistency with those reported
in other studies. In this study the highest ranked item was
the 'lack of authority to change practice'. Interestingly,
this item was also found to be the highest ranked barrier
in several countries which have different health care systems
to Bahrain. The second highest ranked barrier was related
to inadequate facilities. Compared to the other studies, this
was consistent with the Swedish study(22) as well as an Iranian
study.(12) The third highest barrier was the lack of time
to implement new ideas, a similar finding to the study conducted
in Hong Kong.(19)
These findings suggest that organizational
support is imperative to research utilization. Nurses need
to feel empowered to change practices in their clinical setting
and not be constrained by the bureaucratic demands of a hierarchical
organization. According to Mulhall,(24) it is misleading to
dichotomize those carrying out research and those acting in
organizational roles as unrelated; rather they should be seen
in the context of a whole system. There is a need to procure
resources to support and sustain the nurses to increase the
nurses' research activity.
The study conducted among Iranian
nurses(12) reported the lack of time to read research as their
greatest barrier and the lack of authority to change practices
as their third greatest barrier. This may be explained by
a greater number of senior nurses participating in the study.
In this study, 9.1% were ward supervisors and 1.4% were nurse
educators compared to 14.4% head nurses and 8.5% nurse educators
in the Iranian study. Nurses in higher positions within a
hospital hierarchy are likely to have more authority than
those at lower levels and would have higher degrees of autonomy
and empowerment to change practices.(25)
It is not surprising that time constraints
were ranked within the top three, with lack of time to implement
new ideas ranked third, consistent with other studies.(26,
27) Lack of time as a major barrier to research utilization,
reflects a serious long-standing problem that exists world-
wide.(25)
There were several limitations in
this study. This study was carried out in a large teaching
and research hospital; thus the findings may not be generalized
to all Bahraini nurses in other settings. There may be reporting
bias associated with the self-report method which raises questions
about the extent to which the responses accurately represent
all nurses' perceptions of the barriers to research utilization.
The internal consistency of the instrument is relatively low.
Conclusions
This study identified the perceived barriers to research utilization
among Bahraini nurses in a major teaching hospital. The findings
showed considerable consistency with those reported by the
nurses from other countries. In this study, the organization
was a significant barrier to research utilization. The greatest
individual item reported was the lack of authority to change
practice. Although this study found no differences in the
barriers to research utilization compared to other countries,
this is the first study of its kind conducted in Bahrain.
If research utilization is to be enhanced in Bahrain, the
local organizational barriers need to be addressed. An important
step is to create an organizational environment that recognizes
the value of research and encourages and supports nurses'
research activities.
References
1. Olade R. Evidence-based practice and research utilisation
activities among rural nurses. J Nurs Scholarship. 2004;36(3):220-225.
2. Swan B, Al-Gasseer N, Lang N. Global partnerships to strengthen
the evidence-base for nursing. Nurs Econ. 2003;21(5):247-252.
3. Funk S, Champagne M, Wiese R, Tornquist E. BARRIERS: The
barriers to research utilisation scale. Appl Nurs Res. 1991;4(1):39-45.
4. Karkos B, Peters K. A magnet community hospital: fewer
barriers to nursing research utilisation. J Nurs Adm. 2006;36(7):377-382.
5. Brenner M. Children's nursing in Ireland: barriers to,
and facilitators of, research utilisation. Paediatr Nurs.
2005;17(4):40-45.
6. Ashley J. Barriers and facilitators to research utilisation
as perceived by critical care nurses. 2005, University of
California, Department of Nursing.
7. Parahoo K. Barriers to, and facilitators of, research utilization
among nurses in Northern Ireland. JAN. 2000;31:89-98.
8. Andersson N, Jylli L, Kajermo K, Klang B. Nurses in paediatric
care-self-reported professional self and perceived research
utilisation. Scand J Caring Sci. 2007; 21(4):426-433.
9. Hommelstad J, Ruland C. Norwegian nurses' perceived barriers
and facilitators to research use. AORN. 2004;79:621-634.
10. Uysal A, Temel A, Ardahan M, Ozkahraman S. Barriers to
research utilisation among nurses in Turkey. J Clin Nurs.
2010;19:3443-3452.
11. Yava AT, N, Cicek H, Yavan T, Terakye G, Hatipo?lu S.
Nurses' perception of the barriers to and the facilitators
of research utilisation in Turkey. Appl Nurs Res. 2009; 22:166-175.
12. Mehrdad N, Salsali M, Kazemnejad A. The spectrum of barriers
to and facilitators of research utilisation in Iranian nursing.
J Clin Nurs. 2008;17:2194-2202.
13. Mehrdad N, Salsali M, Kazemnejad A. Iranian nurses' attitudes
toward research utilisation. J Res Nurs. 2008;13(1):53-65.
14. Ministry of Health. Bahrain Health Statistics 2007. http://www.moh.gov.bh/PDF/hs2007/hs2007_e.html.
15. Rogers E. Diffusion of Innovation. 5th ed. New York: Free
Press; 2003.
16. Atkinson M, Turkel M, Cashy J. Overcoming barriers to
research in a Magnet Community Hospital. J Nurs Care Qual.
2008;23(4):362-368.
17. Chien W. A survey of nurses' perceived barriers to research
utilisation in Hong Kong. J Clin Nurs. 2010;19:3584-3586.
18. Sari D, Turgay A, Genc R, Bozkurt O. Research activities
and perceptions of barriers to research utilisation among
Turkish nurses. J Cont Edu Nurs. 2012;43(6):251-258.
19. Chau J, Lopez V, Thompson D. A survey of Hong Kong nurses'
perceptions of barriers to and facilitators of research utilisation.
Res Nurs Health. 2008;31:640-649.
20. Brown C, Ecoff L, Kim S, et al. Multi-institutional study
of barriers to research utilisation and evidence-based practice
among hospital nurses. J Clin Nurs. 2010; 19:1944-1951.
21. Kocaman G, Seren S, Lash A, Kurt S, Bengu N, Yurumezoglu
H. Barriers to research utilisation by staff nurses in a university
hospital. J Clin Nurs 2009;19:1908-1918.
22. Boström A, Kajermo K, Nordström G, Wallin L.
Barriers to research utilisation and research use among registered
nurses working in the care of older people: Does the BARRIERS
Scale discriminate between research users and non-research
users on perceptions of barriers? Implement Sci. 2008;3:24-33.
23. Carlson C, Plonczynski D. Has the BARRIERS Scale changed
nursing practice? An integrative review. JAN. 2008;63(4):322-333.
24. Mulhall A. Nursing research: Our world not theirs? JAN.
1997;25:969-976.
25. Veeramah V. Utilisation of research findings by graduate
nurses and midwives. JAN. 2004;47:183-191.
26. Oh E. Research activities and perceptions of barriers
to research utilisation among critical care nurses in Korea.
Intensive Crit Care Nurs. 2008;24:314-322.
27. Vratny A, Shriver D. A conceptual model for growing evidence
based practice.
Nurs Adm Q. 2007;3:162-170.
|
 |

