| |
April
2014
- Volume 8, Issue 2
Effect of Combined
Interventions of Diet and Physical Activity on the Perceived
and Actual Risk of Coronary Heart Disease among Women in North
of Jordan

|
 ( (
|
Muneer Mohammad
Bustanji (1)
Sawsan Majali (2)
(1) Faculty of Nursing, AL-Hussein Bin Talal University,
Jordan
(2) Secretary General Higher Population Council, Jordan
Correspondence:
Dr. Muneer Mohammad Bustanji
Faculty of Nursing, AL-Hussein Bin Talal University,
Jordan
Email: mbustanji@hotmail.com
|
|
|
Abstract
Background and Aim: Women have received little
attention in cardiac research in Jordan. This study
aimed to evaluate the effectiveness of combined interventions
of diet and physical activity on the perceived and actual
risk for coronary heart disease among women in the north
of Jordan.
Methods: An experimental pretest/ posttest design
was used. The sample consisted of asymptomatic women
aged 40 years or older who lived in the north of Jordan.
The intervention involved recommendations concerning
healthy diet and physical activity to modify the actual
risk for coronary heart disease.
Results: The Kruskal-Wallis test; X2(2,
N = 134) = 46.62, p< 0.001, showed that women
who applied both diet and physical activity interventions
scored lower actual risk for heart disease than women
who only applied one type of intervention (either diet
or physical activity).
Conclusion: The results indicated the need for
constant national heart disease education programmes
for women emphasizing adopting healthy lifestyle behaviors.
Key words: Coronary heart disease, Diet, Physical
activity, Women, Risk.
|
Introduction
and Background
Cardiovascular disease (CVD) and stroke are rapidly growing
problems, and are the major causes of illness and deaths in
the Eastern Mediterranean Region, accounting for 31% of deaths
(Khatib, 2004).
Jordanian women were found to underestimate their risk for
coronary heart disease (CHD); and perceived breast cancer
as a greater risk to their health than CHD (Ammouri, et al.,
2010). Despite that, 28.9% of deaths among women in Jordan
were attributed to CHD and 23.5% were due to breast cancer
(JMOH, 2011). The majority of research on Jordanian women's
health has focused exclusively on reproductive health aspects
(AL-Qutob, 2001) and screening for breast cancer (Petro-Nustus
and Mikhail, 2002), and so far no study has been performed
which investigates the perceived and the actual risk of coronary
heart disease and or interventions that could reduce the risk
of CHD among women in Jordan.
This study aimed to assess the perceived risk and the actual
risk for coronary heart disease among women in the north of
Jordan. This study also aimed to evaluate the effectiveness
of combined interventions of diet and physical activity on
the perceived and actual risk for coronary heart disease among
women in north of Jordan.
Research Methods
Setting and Sample
A true experimental pretest/ posttest study was conducted
among a convenience sample of women who visited the out-patients
department at a university hospital and at a government hospital
(hospitals are located in the Irbid governorate). The inclusion
criteria of the sample were age is equal to or more than 40
years, willing to participate and not known to have CHD. The
sample size was estimated using power analysis which yielded
a sample size of 159 participants. In this study, the researcher
gathered data from 165 women to avoid the attrition risk.
Procedure
Phase One: Pretest Phase
After obtaining the approval to conduct the study from the
Committee on Human Research, the Jordanian Ministry of Health,
and the university hospital, the researcher visited the out-patient
department of each setting, where the women were invited to
participate in the study. Those who accepted to participate
in the study were asked to read and sign the informed consent
form. The form explained the purpose of the study, supplied
the woman with information about her rights as a participant,
and included directions for completing each of the forms.
In adherence with ethical standards, the informed consent
form also included information regarding confidentiality,
the intervention involved in the study, and a statement regarding
the participants' ability to withdraw from the study at any
time without penalty.
After signing the informed consent form, each woman completed
the survey forms; Demographic information sheet, and the Perception
of Risk of Heart Disease Scale (PRHDS). The PRHDS is a newly
developed and previously tested 20-item questionnaire composed
of three subscales: dread risk, risk and unknown risk (Ammouri
and Neuberger, 2008). These subscales are intended to place
individuals on a continuum from low perception of risk to
high perception of risk of CHD.
Dread risk, was defined at its high end as perceived lack
of control, dread, catastrophic potential, fatal consequences;
while unknown risk, was defined at its low end as perception
of hazards judged to be unobservable, unknown, new and delayed
in their manifestation of harm; and (in between) risk reflecting
a hazard that has few moderate known outcomes and consequences
(Ammouri and Neuberger, 2008).
Items were formatted using a four-point Likert scale ranging
from 1-4 (strongly disagree to strongly agree). To score the
instrument, item scores were summed for each subscale, as
well as across subscales for a total scale score; reverse
scoring of negative-response items is required (Ammouri and
Neuberger, 2008). Higher scores on the PRHDS subscales indicate
a higher perception of risk of CHD. Cronbach's alpha internal
consistency reliability coefficients of the original PRHDS
were .80, 0.72 and 0.68 for the dread risk subscale, the risk
subscale, and the unknown risk subscale respectively, with
a total scale reliability of .80 (Ammouri and Neuberger, 2008).
A test-retest correlation coefficient was also calculated
for the original version and yielded a total reliability of
0.72 with 0.76 for the dread risk subscale, 0.70 for the risk
subscale, and 0.61 for the unknown risk subscale (Ammouri
and Neuberger, 2008).
After completing the surveys forms, the researcher carried
out the physiologic measures (body height, body weight, blood
pressure, and blood glucose level). After weighing each woman
with the same scale, the researcher calculated the body mass
index of each woman using the results of height and weight
measurements.
Regarding measuring blood pressure, the researcher measured
the BP for each participant after ten minutes rest. Two independent
measurements of blood pressure were obtained with an interval
of at least ten minutes between them and the average BP was
calculated. For the purpose of this study, hypertension (HTN)
was defined as a person having a blood pressure equal to or
more than 140/90 mmHg or those individuals who are on antihypertensive
agents (AHA, 2010; National Institute of Health, 2002).
Regarding measuring blood glucose level, the researcher used
an Accu- Check machine, test strips, lancets, gloves, and
biohazard container. For the purpose of this study, a person
who has diabetes is defined as someone taking insulin or oral
hypoglycemic drugs, or with a fasting plasma glucose concentration
above 7.0 mmol/l (126 mg/dl).
After measuring the physiologic measures, the researcher used
the WHO/ISH risk prediction chart of the EMRO- B region without
cholesterol level to estimate the actual risk of CHD among
women (Figure 1). To estimate the actual risk using these
charts, the researcher collected data about the items included
in the charts; age, smoking status (all current smokers and
those who quit smoking less than one year before the assessment
were considered smokers for assessing cardiovascular risk),
blood pressure, and presence of diabetes mellitus. Then, the
researcher classified each participant into a category of
high risk (30% to <40% and >40%; red and maroon
color), medium risk (from 10% to <20% and from 20% to <30%;
yellow and orange), or low risk (<10%; green color) for
heart attack or stroke in the following ten years.
Click here for Charts
Phase Two: Intervention Phase
In this phase, the researcher randomly assigned the participants
into three groups (A, B, and C) and randomly also assigned
the interventions (diet and physical activity, diet part only,
or physical activity part only) to the groups. Eventually,
group A was assigned to the diet part of the intervention,
group B was assigned to both diet and physical activity interventions,
and group C was assigned to the physical activity part of
the intervention.
In this study, group B acted as the experimental group and
received both components of the intervention and group A and
C acted as the control groups and received only one component
of the intervention; either physical activity or diet component.
The researcher then provided a presentation for group A about
how to prevent CHD using the diet intervention only, a presentation
for group B about how to prevent CHD using both diet and physical
activity interventions, and a presentation for group C about
how to prevent CHD using physical activity intervention only.
Finally, the researcher emphasized to the women the importance
of following the guidelines for 12 weeks. Each four weeks
of this phase, the researcher contacted the participants in
order to make sure that they were committed to the guidelines
and to discuss any inquiry they had. Participants were contacted
via mobile phone.
Phase Three: Posttest Phase
After 12 weeks, the women individually returned to the out-patient
clinic to be reassessed for their physiologic measures and
to complete the PRHDS.
Educational Materials
The educational material was developed based on the "Pocket
guidelines for assessment and management of cardiovascular
risk with the WHO/ISH cardiovascular risk prediction charts
for WHO epidemiological sub-regions EMR- B, EMR- D" (WHO,
2007). The content of educational material was on how to prevent
occurrence of coronary heart disease through following specific
recommendations regarding diet and physical activity.
Regarding the recommendations about diet changes, women at
risk for CHD were strongly encouraged to reduce total fat
and saturated fat intake. In addition, they were strongly
encouraged to reduce daily salt intake by at least one-third
and, if possible, to <5 g per day. The women were encouraged
to eat at least 400 g a day, of a range of fruits and vegetables,
as well as whole grains. In addition, the women were strongly
encouraged to take at least 30 minutes of moderate physical
activity (e.g. brisk walking) a day, through leisure time,
daily tasks and work-related physical activity.
Results
Sample Characteristics
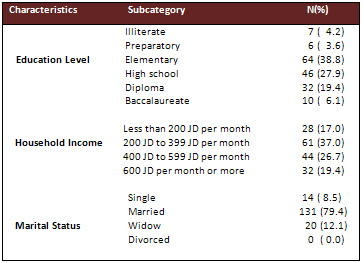
Table 1 shows the demographic characteristics of the sample.
The mean age of the women in the sample was 52.6 (SD = 4.4)
ranging from 41 to 69 years. About 79.4% of the participants
were married, and the monthly household income of 17.0% of
the participants was less than 200 JD. More than half of the
women (53.4%) had a high school education or higher.
Table 1: Demographic Characteristics of the Sample (N =
165)
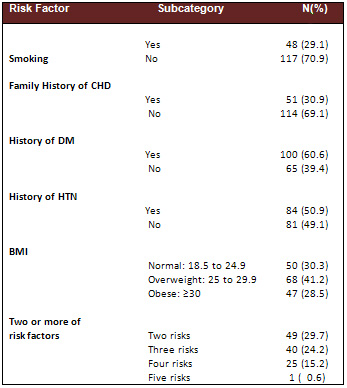
Risk Factors for CHD
The results indicated that 29.1% of participants were smokers,
30.9% had a family history of CHD, 60.6% were known to have
DM, 50.9% were known to have HTN, and 28.5% were obese (BMI
> 30). In addition, 69.7 % of the participants had multiple
risk factors for CHD (Table 2).
Table 2: Risk Factors for CHD (N= 165)
Level of Perceived Risk and the Actual Risk
Table 3 provides data about the level of perceived risk among
the participants at the pretest phase of the study. The results
show that the mean score of total perceived risk was 49.7
out of 80.0, ranging from 33 to 71.
Table 3: Mean, Median, and Standard
Deviation of Perceived Risk at Pretest (N= 165)
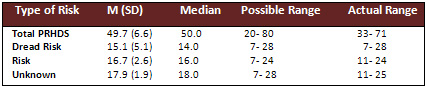
Table 4 shows data about the level of perceived risk among
the participants at the posttest phase. Note that, 31 women
from the original sample (N= 165) apologized for participating
in the posttest phase. The results show that the mean score
of total perceived risk was about 54.0 out of 80.0, ranging
from 40 to 72(N = 134). Whereas, the mean score of total perceived
risk for the same group (N = 134) was 48.6 out of 80.0 at
pretest phase.
Table 4: Mean, Median, and Standard Deviation of Perceived
Risk at Posttest (N= 134)

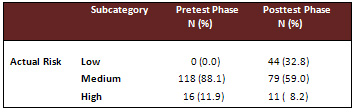
Regarding the level of the actual risk among participants
(Table 5), 32.8% of participants were at a low level of actual
risk for CHD according to the WHO/ ISH prediction charts.
Table 5: Percentages of Actual Risk (N= 134)
To evaluate the impact of intervention on the perception
level, a Paired sample t test was conducted to estimate the
difference in the mean score of the level of perceived risk
for CHD from the pretest and posttest phases of the study.
The results showed that there was a statistically significant
increase in the perception for CHD between the pretest phase
(M = 48.6, SD = 6.0) and the posttest phase (M = 54.0, SD
= 6.1), t (133) = -23.543, P<.0001. Since, the mean increase
was 5.4 with a 95% confidence interval ranging from 4.9 to
5.8, in addition, a Wilcoxon Signed Rank test was conducted
to evaluate the difference in the level of actual risk among
participants from the pretest and posttest phases of the study.
The analysis revealed a statistically significant reduction
in risk for CHD following participation in the program, Z
= - 6.486, P<0.001.
A Kruskal-Wallis test was conducted to evaluate differences
among the three types of interventions (diet only, diet and
physical activity, and physical activity only) on median change
in the level of actual risk for CHD. The test, which was corrected
for tied ranks, was significant X2(2,
N = 134) = 46.62, p< 0.001. The Mann-Whitney U test was
conducted to evaluate pairwise differences among the three
types of interventions, controlling for Type I error across
tests by using the Bonferroni approach. The results of these
tests indicated a significant difference in the level of actual
risk between the group who implemented both interventions
(diet and physical activity) and the group who only implemented
the diet intervention (U= 441.5, p< 0.001). Also, there
was a significant difference in the level of actual risk between
the group who implemented both interventions (diet and physical
activity) and the group who implemented the physical activity
intervention (U= 302.5, p< 0.001). Therefore, implementing
both interventions (diet and physical activity) elicited statistically
lower level of actual risk than implementing only one type
of intervention (p< 0.001). Note that, there was no statistically
significance difference in the level of actual risk median
between the group who implemented the diet intervention and
the group who implemented the physical activity intervention
(U= 922, p= 0.051).
Discussion
Perceived Risk of Heart disease
Several studies have found that a majority of women underestimated
their risk of heart disease (Lefler, 2004; Mosca, et al.,
2000; Mosca, et al., 2006, Ammouri, et al., 2010). This study
supports the work of others in pointing out the lack of awareness
among women about their susceptibility to this disease. In
the view of this fact, the mean of total score of the PRHDS
among women in this study was consistent with the mean of
total score of the PRHDS among participants in a study conducted
in Jordan by Ammouri, et al., (2010); of 43 out of 80 ranging
from 20 to 57. In addition, the mean score of unknown subscale
in this study was 17.9 out of 24 which corresponded with results
reported by Ammouri, et al. (2010); of 14.4 out of 24. These
results indicated that participants tend to downplay their
risk of heart disease.
Intervention
The results of the effectiveness of combined diet and
physical activity interventions that have been used in this
study are analogous to the results of other studies. Muto
and Yamauchi (2001) conducted a workplace health promotion
program targeting diet and exercise to reduce CVD risk among
152 employees in which the intervention group spent four days
at a resort for intensive lectures and training. The participants
were assessed at baseline and at three month intervals for
one year after the program. Those in the intervention group
showed significant improvements in body mass index, and systolic
blood pressure. Similarly, a 12 week employee wellness pilot
program involving university employees (N = 50) focused on
reducing risk factors for CHD through interventions aimed
at improving diet and implementing a consistent exercise regimen
(White and Jacques, 2007). The study's participants attended
monthly workshops and had pre- and post-intervention measurements,
which included weight, body composition, BP, TC, LDL-C, HDL-C,
TC/HDL-C ratio, TG, and blood glucose (White and Jacques,
2007). A significant difference was observed between pre-
and post-intervention measurements of weight (p = .01) (White
and Jacques, 2007). However, statistically significant improvement
was not seen in blood pressure. They also confirmed that only
25 of the original 50 participants remained (50%) at post-test,
which potentially skewed the results of an already miniscule
sample size (White and Jacques, 2007).
Limitations
One of the limitations of this study was the use of a
convenience sample which may not be truly representative of
women in Jordan. Although recruitment took place at several
local hospitals, generalizability is limited due to geographic
and nonrandom sample selection. Also, about 19% of participants
did not complete the post test phase.
Recommendations
Recommendations for Future Research:
• Conduct additional studies to include women with
less education, as well as women from different regions and
age categories.
• Conduct additional studies that include practical training
of the recommendations before starting the actual program.
• Conduct additional studies that include the WHO/ISH
risk predictions charts with cholesterol.
• Conduct qualitative research to understand why women
do not perceive themselves susceptible to heart disease and
why they do not practice behaviors that could reduce their
risk of developing heart disease and promote overall wellness.
Recommendations for Health Education Practice:
• There is a need for an increase in education regarding
personal risk factors for heart disease and devising strategies
to increase perceived susceptibility to the disease. It is
imperative that nurses help resolve common misperceptions
women have about heart disease and create increased awareness
of the disease. Current awareness campaigns have achieved
greater recognition of the impact of heart disease, but a
gap in awareness continues to exist. This gap might be narrowed
with more emphasis on social marketing through a media (i.e.,
television) available to the majority of the population.
• Exploration of the role of the physician recommending
heart disease screening is needed. In an effort to increase
screening behaviors of women, nurses can play a key role,
acting as a resource for both physicians and the community.
Nurses can help direct all women, whether they perceive themselves
as susceptible or not, to appropriate screening tests for
heart disease. Targeting younger women and those with lower
education levels also is necessary to reach a population that's
often under-represented in screenings.
• Health professionals, marketing experts, and non-profit
organizations, such as the Jordan Nursing Council, need to
collaborate to gain a better understanding of the priority
population's beliefs about heart disease and motivation to
participate in health-promoting behaviors to decrease risk
factors for heart disease. Marketing campaigns can be developed
to personalize the disease so women can relate to and understand
their vulnerability to the condition.
Conclusion
Cardiovascular risk factors should be assessed in women
starting much earlier than menopause and should then be treated
as aggressively in women as in men. Few women appreciate that
cardiovascular disease is their major health problem. So,
any woman can benefit from increased awareness of her risks,
and the younger women who adopt healthy lifestyle behaviors
now may avoid developing heart disease later in life.
References
1. Khatib O. Noncommunicable
diseases: Risk factors and regional strategies for prevention
and care. The Eastern Mediterranean Health Journal, 2004,
6: 778- 788.
2. Ammouri A, Neuberger G, Mrayyan
M, Hamaideh, S. Perception of risk of coronary heart disease
among Jordanians. Journal of Clinical Nursing, 2010, 20: 197-
203.
3. Mortality data in Jordan 2008.
Jordan Ministry of Health, 2011. (http://www.moh.gov.jo/MOH/En/publications.php/
accessed 20 June 2011).
4. Qutob R. Menopause- associated
problems: types and magnitude. A study in ain al-basha area,
Jordan. Journal of Advanced Nursing, 2001, 33: 613- 620.
5. Petro-Nustus W, Mikhail B. Factors
associated with breast self examination among Jordanian women.
Journal of Public Health Nursing, 2001, 19: 263-271.
6. Ammouri A, Neuberger G. The perception
of risk of heart disease scale: Development and psychometric
analysis. Journal of Nursing Measurement, 2008, 16: 83-97.
7. Heart disease and stroke Statistics
2010 Update. American Heart Association, 2010. (http://circ.ahajournals.org/cgi/reprint/121/7/e46/
accessed 8 June 2011).
8. The National Cholesterol Education
Program Adult Treatment Panel III (NCEP ATP III) 2001. National
Institute of Health, 2002. (http://www.nhlbi.nih.gov/guidelines/cholesterol/atp3full.pdf/
accessed 2 August 2011).
9. Pocket guidelines for Assessment
and Management of Cardiovascular Risk with the WHO/ISH Cardiovascular
Risk Prediction Charts for WHO epidemiological sub-regions
EMR- B, EMR- D. World Health Organization, 2007. (http://www.who.int/cardiovascular_diseases/guidelines/PocketGL.ENGLISH.AFR-D-E.rev1.pdf/
accessed 2 August 2011).
10. Lefler L. Perceived risk of heart
attack: A function of gender? Nursing Forum, 2001, 39: 18-26.
11. Mosca L et al. Awareness, perceptions,
and knowledge of heart disease risk and prevention among women
in the United States. Archives of Family Medicine, 2000, 9:
506-515.
12. Mosca L et al. National study
of women's awareness, preventive action, and barriers to cardiovascular
health. Circulation-Journal of the American Heart Association,
2006, 113: 525-534.
13. Muto T, Yamauchi K. Evaluation
of a multi-component workplace health promotion program in
Japan on CVD risk factors. Journal of Preventive Medicine,
2001, 33: 571-577.
14. White K, Jacques P. Combined
diet and exercise intervention in the workplace: Effect on
CVD risk factors. American Association of Occupational Health
Journal, 2007, 55: 109-114.
|
 |

