| |
April
2014
- Volume 8, Issue 2
Menopausal
Women's Sexual Function and Related Factors in West of Tehran

|
 ( (
|
Mina Amiri
Pebdani (1)
Simin Taavoni (2)
Hamid Haghani (3)
(1) Instructor & Faculty Member, Department of Midwifery,
Faculty of Medicine, Alborz University of Medical Sciences,
Iran
(2) Senior Lecturer & Researcher, Nursing and Midwifery
Faculty, Tehran University of Medical Sciences (TUMS),
PhD Student in Medical Education, Faculty of Medicine,
TUMS Member of Research Institute for Islamic &
Complementary Medicine (RICM) (TUMS), Tehran, Iran
(3) Senior Lecturer, School of Management & Medical
Information Science, TUMS, Tehran of Medical Sciences,
Iran
Correspondence:
Simin Taavoni
Instructor & Faculty
Member, Department of Midwifery, Faculty of Medicine,
Alborz University of Medical Sciences, Iran
Telefax: 009821 66921228
Email: staavoni14@yahoo.com
|
|
|
Abstract
Background: A lot of progress has been made in
prevention and treatment of menopausal problems but
still sexual function, which may be influenced by several
factors, need more attention. It is essential to identify
these factors in this period.
Aim: To assess related factors of sexual functioning
in postmenopausal women.
Materials and Methods: In this descriptive cross-sectional
study, 163 volunteer healthy married postmenopausal
women, who had been visited in selected health centers
in west of Tehran, were enrolled. Data was collected
by using demographics questionnaire and Sabbatsberg
Sexual Rating Scale (SSRS). Data were analyzed by using
independent t-test, ANOVA and Pearson correlation coefficient.
This study was approved by the Ethics Committee of Tehran
University of Medical Sciences (TUMS).
Results: The results showed that sexual function
had a significant relationship with employment status,
educational level, number of children, number of children
at home, frequency of sexual intercourse per month and
sexual satisfaction. On the other hand, sexual dysfunction
had no significant relationship with women's age, husband's
age, age of menopause, duration of marriage, number
of children and economic status.
Conclusion: Sexual function in the postmenopausal
period can be influenced by some social and personal
characteristics. By understanding and knowing these
characteristics, Health care providers could prepare
suitable guiding and counseling for each target group
for improving their sexual function and quality of life.
Key words: Sexual function; Menopause; Sabbatsberg
Sexual Rating Scale (SSRS)
|
Background
According to the report by World Health Organization,
menopause begins 12 months after spontaneous cessation of
menstruation as a result of inactivity of ovaries, which is
accompanied by hormonal, biological and clinical symptoms
(1) and today due to health care improvement and increased
life expectancy, women spend a considerable time in this period
(1-4). According to Iran's yearbook of statistics in 2007,
13.87 Percent of women were 45 to 60 years old (5). Menopause
symptoms can be classified into three categories of vasomotor
symptoms such as hot flash and night sweat, central symptoms
such as insomnia and changes in memory and concentration and
genitourinary symptoms such as vaginal dryness, dyspareunia,
urinary tract infections and urinary incontinence (6).
Although a lot of progress has been made in prevention and
treatment of menopausal symptoms till the end of 20th Century,
what seems to have received little attention in this regard
was sexual function and its related problems (7), while sexual
function constitutes an important part of women's health,
sense of well-being (8-10) and affects their quality of life
(9). Despite the great importance of healthy sexual function,
many studies have indicated some problems in this regard (11).
A cross-sectional study in the U.S. (2004) on women over 50
to 79 years old reported that prevalence of vaginal dryness
and dyspareunia among the studied women was 27% and 5.2%,
respectively. Also a study in six European countries (2008)
of reduced sexual activity of 50-60 years old postmenopausal
women, was reported in 34%, and showed effect of age on it
(2). Beigi et al. (2009) reported frequency of sexual dysfunction
during menopause period as 72.4% (12). The prevalence of these
complaints increases with rising age (13). The main causes
of sexual dysfunction in this period include physiological
changes, psychological problems (14) and lack of sexual knowledge.
These factors make the critical menopause period very risky
because sexual disorders also mutually lead to reduced mental
health of families through causing or exacerbating psychological
problems (15). Regarding the Lopez study (2012), in a mid-aged
Spanish sample, lower sexual function was related to menopausal
and mood symptoms, several women and partner factors. Also
they emphasized that further research is needed. (16) Regarding
the Aida et al (2013) study, characteristics of the menopausal
women that were statistically significant in those with sexual
dysfunction were age, educational, race, and type of menopause.
(17)
Considering the prevalence of sexual dysfunction in the menopause
period and importance of maintaining sexual relations in this
period, it is always important to have more study in this
field (18). Since there was no documented study in the field
of assessment of sexual function and related factors in menopausal
women in Tehran, this study was carried out, to improve the
health status of this vulnerable group of society.
Materials and Methods
In this cross-sectional study, which had been approved by
the Research Ethics Committee of Tehran University of Medical
Sciences (TUMS), and carried out in the selected health centers
in west of Tehran, 163 volunteer healthy postmenopausal women
aged 50- 60 years old were involved during year 2011-2012.
The subjects of the study were invited for a screening project
of hypertension and diabetes. The subjects were recruited
from the community through newspaper ads, flyers, and the
internet, also their eligibility was assessed by using structured
interview.
The inclusion criteria were age 50- 60 years old, passing
at least one year since menopause, not taking hormone replacement
therapy, not having physical or mental diseases in women and
their husbands, including diseases which affect sexual function,
such as vasculitis, cardiovascular diseases, mental diseases,
neurological disorders, thyroid problems and cancers, no taking
drugs that affect sexual function such as anti cholinergic
drugs, psychotropic, neurology drugs and hormones, no recent
stresses such as unfaithful spouse, death, serious diseases
or imprisonment of close friends and relatives in the past
year, not separated from spouse during the interview, not
suffering from premature ejaculation or impotence among their
husbands, being illiterate and having at least one intercourse
during previous month.
The assessment of the study included two main parts. In the
first part personal characteristics, including age, time of
last menstruation, number of coitus, number of children, number
of children in home, education, occupation, and economic status
of the volunteers, and spouse age. In the second part Sabbatsberg
Sexual Rating Scale (SSRS), which is a valid and reliable
questionnaire (19) and its Persian version has been previously
used in various studies in Iran (20, 21), measure sexual function
by assessing the domains of sexual desire, activity, satisfaction,
arousal or pleasure, orgasm, and the importance of sex. Each
domain have two items, therefore it has six for assessing
different aspects of sexual function in the previous month,
while the others assessed different aspects of sexual function
in comparison to previous years. The response options were
on a 5- point Likert scale rating system and the responses
to each question were summed and converted to a percentage,
producing a "sexual rating" between zero and 100.
After a detailed explanation of the procedure of study, written
informed consent was obtained from the subjects, then, they
filled out questionnaires of personal information and SSRS.
Finally, the scores were calculated and analyzed by independent
t-test, ANOVA and Pearson correlation coefficient (a
was considered 0.05). All the statistical analyses
were performed using SPSS16 software.
Results
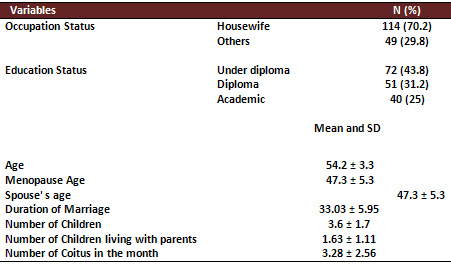
The mean age of menopause in study subjects was 48.1±
4.1. Most of the participants (42.9%) were 50- 52 years old,
and had one or two times of sexual intercourse per month (49.2%).
The majority of women (41.4%) had a high school diploma, 69.9%
were housewives and 65.1% had a moderate economic status.
The mean age of their husbands was 59.41 ± 5.2. (Table
1)
Table 1: Personal characteristics
The relationship of the considered factors and sexual function
was as follows: according to independent t-test, ANOVA and
Pearson correlation, women's employment status (p<0.01),
educational level (p<0.001), number of children (p<0.02),
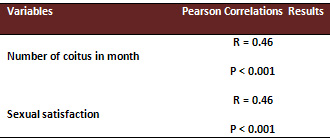
number of children at home (p<0.03), frequency of sexual
intercourse per month (p<0.001) and their sexual satisfaction
(p<0.001) had a significant relationship with sexual function
(Tables 2 -3). According to the relationship between educational
level and sexual function, the results of Scheffe test demonstrated
Sexual function of those who had academic education was better
than others (p<0.02). On the other hand, sexual dysfunction
had no significant relationship with women's age, husband's
age, menopause age, duration of marriage, number of children
and economic status.
Table 2: Variables, Sexual Function and Test Results
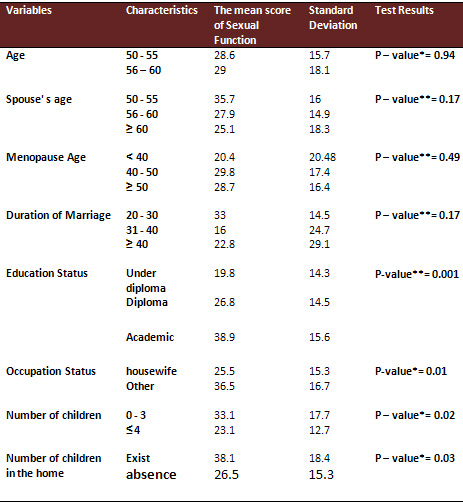
Independent Samples Test
**ANOVA
Table 3: Number of coitus, Sexual satisfaction, Sexual Function
and Test Results
Discussion
Sexual function is a complex combination of physical,
mental and environmental factors (22). In this study in opposition
of Castelo (2003) (23) and Beigi et al (2008) (12) there were
no correlations between age and sexual function. Referring
to correlation between Educational Level and Occupational
status, with sexual function our result was similar to Beigi
et al (12) and Denerestain et al(2003) (24) and referring
to correlation between economical staus, our results were
like Beigi et al, (12) and Gerber Et al. (25).
Conclusion
Sexual function in postmenopausal period can be influenced
by some social and personal characteristics. By understanding
and knowing these characteristics, Health care providers could
prepare suitable guiding and counseling for each target group
for improving their sexual function and quality of life.
The results of the present study indicated the effect of factors
such as level of education, employment, number of children,
number of children at home, frequency of sexual intercourse
and sexual satisfaction on sexual function. Undoubtedly, having
adequate sexual knowledge plays a key role in improvement
of sexual function in such women. The effect of sexual knowledge
was not studied in this paper, since women with an academic
degree showed better sexual function. Hence, it can be recommended
for the staff of health care centers to remind postmenopausal
women about their development with age and reaching the time
of menopause and the importance of sexual function in their
life. Thus, they should hold continuous training courses by
qualified instructors and experts in order to improve sexual
knowledge and health of these target groups for improving
their quality of life.
Acknowledgements
The authors would like to thank the Research Chancellor
of Tehran University of Medical Sciences for delivering financial
support for process of this study. This study had been approved
by Ethics Committee of Tehran University of Medical Sciences,
also is the first phase of study, which had been registered
in Iranian Registry of Clinical Trials, which is a Primary
Registry in the WHO Registry Network set up with the help
from the Ministry of Health and Medical Education (MOHME)
of Iran. (Registry Number: N5 201010192172)
Authors would also like to thank Andrea Garratt for providing
valuable information about SSRS.
References
1. Berek J: Berek & Novak Gynecology. Vol 2,
14 edit. Philadelphia. 2007; 1063 - 74
2. Nappy R, Lachowsky M. Menopause and sexuality: Prevalence
of symptoms and impact on quality of life. Maturitas.2009
;23: 4
3. Cheema D, Coomarasamy A, Toukhy T. Non hormonal therapy
of post-menopausal vasomotor symptoms: a structured evidence-based
review. Arch Gynecol Obstet. 2007; 276: 463-469
4. Al-Azzawi F, Palacios S. Hormonal changes during menopause.
Maturitas. 2009;63: 135-137
5. National Portal of Statistics, General Population Census
tables housing choice, 1385. http://www.sci.org.ir
6. Hickey M, Saunders C, Stuckey B. Non-hormonal treatments
for menopausal symptoms. Maturitas.2007; 57: 85- 89
7. Bonnie R, Saks MD. Sexual dysfunction (Sex, drugs, and
women's Issues). Primary care up date for OB/GYNS;1999, 6(2):61-5
8. Mimoun S, Wylie k. Female Sexual Dysfunction. Definitions
and classification. Maturitas. 2009; 63 (2): 117-118. http://www.elsevier.com/locate/maturitas
9. Valadares AL, Pinto-Neto AM, Conde DM, Osis MJ, Sousa MH,
Costa-Paiva L. The sexuality of middle-aged women with a sexual
partner: a population-based study. Menopause 2008;15 (4):706-713
10. Gracia C, Freeman E, Sammel M, Lin H, Mogul M. Hormones
and Sexuality during Transition to Menopause. Obstetrics &
Gynecologists.2007; 109(4):831-840
11. Basson, R. Berman, J. Burnet, A. Derogatis, L. Ferguson,
D. Fourcroy, L et al. Report of the interventional consensus
development conference on female sexual dysfunction. Definition
and classifications. J of urology. 2000; 163: 888 -893
12. Beigi M, Fahami F, Hassanzahraei R, Arman S. Associative
factors to sexual dysfunction in menopause women. Iranian
J of Nursing and Midwifery Research 2008; 13: 32 -35 (Persian)
13. Castelo Branco C. Prevalence of sexual dysfunction in
a cohort of middle-aged women. Obstet Gynaecol 2003; 23(4):420-30.
14. Badawy AZS. Clinical management of the perimenopause.
Sydney: Arnold; 2005.p.46-8.
15. Block A. Self awareness during the menopause. Maturias
2002; 41(3):61-68.
16. Lopez P, Faustino R, Alonso F, Anam M, Pastor T, Martina
M. Assessment of sexual function and related factors in mid-aged
sexually active Spanish women with the six item female sex
function index. Menopause 2012; 19(11): 1224-1230
17. Shimatul Y, Lim C, Soon R, Hatta S. Prevalence of Sexual
Dysfunction and Related Risk Factors for Sexual Dysfunction
among Postmenopausal Malaysian Women Attending Gynaecological
Clinic in Obstetrics & Gynaecology Department of Sabah
Women and Children Hospital. Journal of Surgical Academia
2013 3(1):
18. Taghizadeh Z, Rezaeepour A, Kazemnejad A, Mirsaeidi Z.
The effect of Vitaxnus on effect on menopausal symptoms. School
of Nurse and Midwifery. Tehran University of Medical sciences.
Bahar. 2006; 12 (1): 67 (Persian)
19. Garratt AM, Torgerson DJ, Wyness J, Hall MH, Reid DM.
Measuring sexual functioning in premenopausal women. British
Journal of Obstetrics and Gynaecology 1995;102: 311-6.
20. Taavoni S, Unesi M, Shahpoorian F, Mahmoodian M. Association
of hormone replacement therapy in postmenopausal women with
sexual status of the North Tehran. Thesis for the degree of
Master of Midwifery, School of nursing and Midwifery of Iran,
1999 (Persian)
21. Taavoni S, Anisi B, Ahmadi Z, Hoseini F. Changes in sexual
function in nulliparous women, 6-3 months after delivery of
the relevant factors in the area West of Tehran. Thesis for
the degree of Master of Midwifery, School of nursing and Midwifery
of Iran, 2005 (Persian)
22. Beutel ME. Sexual activity, sexual and partnership satisfaction
in men-results from a German representative community study.
Andrologia 2002; 34(1) :22.
23. Castelo C. Prevalence of sexual dysfunction in a cohort
of middle- aged women. Obstet Gynaecol 2003; 23(4):420-30
24. Dennerstein L. Factors affecting sexual Functioning of
women in the mid- life years. Climacteric 2003; 2(4):245-62.
25. Greber R. A study of premenopausal sexual satisfaction
and other factors contributing to positive or negative expectation
of natural menopause. Fertility and sterility 2004; 76(3):526.
|
 |

